Why a Toolkit?
The principal goal of Together4RD is to stimulate scientific collaborations between European Reference Networks (ERNs) and Industry. Achieving this goal entails overcoming a variety of historical barriers hampering interaction in this space, by adopting a multi-pronged approach centred upon pilots (the learnings from which should foster more -and more varied forms of- collaboration in future). The Together4RD Position Statement, published in Orphanet Journal of Rare Disease in 2023, explored the multifaceted reasons for a general lack of collaboration in this space (whilst also highlighting case studies of fruitful collaborations in the public-private rare disease arena and models for collaboration, before introducing how Together4RD is seeking to move the needle here.). As the Position Statement explains, alongside more policy-oriented ‘barriers’ (real or perceived) such as the Board of Member States Statement of 2019, a range of practical obstacles or uncertainties have limited ERN engagement with Industry:
- for some ERNs, coming from fields with a traditional lack of R&D in the rare disease space, there is a lack of practical knowledge on how to work with Industry.
- there is sometimes a lack of awareness around the kinds of projects ERNs and Industry could collaborate on.
- ERNs are not well known or understand by many companies, and not all actors within ERNs (centred on academics, clinicians and patients) understand the needs and realities of the private sector.
- even where a community is relatively mature, research-wise, challenges arise when it comes to entering into discussions for public-private-collaborations, with often quite different needs and expectations creating bottlenecks and delays.
Whilst other strands of work within Together4RD seek to address the more policy-related challenges hampering ERN and Industry collaboration (for instance, exploring whether a revision of the 2019 BoMS Statement would make sense, and advocating for more opportunities to support Industry-ERN interaction), it was agreed that the initiative should create a Toolkit, to provide practical support for future ERN-Industry collaborations. This was deemed by the Steering Group, and wider community, to be a very valuable activity, particularly in the light of the experiences around launching the first three pilots.
What kind of activity is this Toolkit intended to support?
The Together4RD Toolkit is intended to support a broad range of collaborative activities in which ERNs and Industry might partner. The 2023 Position Statement outlined a range of activities which working groups felt would be appropriate for ERNs and Industry collaboration, and would yield added-value, which have been elaborated further across the course of 2024 into the tool above. This toolkit is mainly concerned with these kinds of activities, more so than traditional clinical trials and partnering in initiatives funded by programmes like the Innovative Healthcare Initiative (IHI).
Core principles underlying the creation of this Toolkit
In setting out to produce this Toolkit, Together4RD centred the activities on 3 core principles:
It is important to avoid ‘reinventing the wheel’:
Where existing resources (such as webpages, reports, publications, guidelines, webinar recordings, templates, etc) serve an important purpose in line with our central mission, this ToolKit links directly to these, rather than seeking to develop very similar resources anew. Where the community has identified gaps and proposed resources which would be beneficial but did not exist, entirely new resources have been created. It is particularly important to consider what is unique about ERN and Industry interactions, vs any and all research activity an academic, say, might enter into.
This Toolkit would best be viewed as an iterative document
This is the first iteration of a Together4RD Toolkit to support and streamline ERN and Industry collaboration. Changing needs and realities in future may necessitate additions to the toolkit. Furthermore, some of the types of tool proposed for inclusion in the course of the 2024 consultations, would require further work and wider stakeholder engagement – for instance, in agreeing model contract clauses to facilitate collaborations between ERNs and Industry. Ideally, therefore, this should be viewed as a dynamic resource which will evolve over time, developing in a stepwise approach, by whichever organisation or initiative is in a position to do so.
Related Resources
This Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceThe process of scoping potential content for this Toolkit began in earnest in Q1 of 2024, via a survey directed to both ERNs and Industry, intended to:
- capture examples of any collaborative activity to-date; and
- attempt to prioritise the importance and usefulness of a range of categories of resources, for fostering ERN-Industry collaboration.
Simultaneously, Together4RD ran a similar poll via social media, to try to assess how valuable different types of resources might be. Also in Q1 of 2024, interviews were conducted with both the ERN and Industry representatives involved in the three Together4RD pilot projects and all relevant insights from those interviews, concerning practical tools and resources that could realistically be incorporated to a toolkit, were noted (see also Tool 9: Experiences and learnings from the first ERN-Industry pilots supported by Together4RD).

categories, which form a starting point for the selection of toolkit domains:
- Background knowledge – to support conceptualisation of a collaborative idea or
research question - Practical knowledge transfer – to progress from an idea to a well-developed research collaboration
- Legal framework
- Testimonials (this was later merged with the ‘Background Knowledge’ domain)
- Existence/creation of third-party brokers to facilitate the collaboration
Targeted consultations – workshops for the academic/clinical research
community and Industry communities
Building on the survey and social media polls, Together4RD organised a broad consultation across May and June, in the form of two workshops.
Firstly, a half-day workshop was organised Bari on 29th May, aimed primarily at the research/ clinical academic community. The workshop ultimately involved 25 experts, largely from academic/researcher backgrounds, some formally engaged with ERNs, others not. After initial presentations contextualising this activity, the group engaged in a brainstorming session to do the following:
- Consider the relevance/appropriateness of the 5 domain headings above, and brainstorm on the types of items which might be included as useful and important examples under each domain.
- Consider what might be missing, which would help support more -and more effective- ERN-Industry collaborations in the future.
- Suggest concrete existing examples of the kind of tools the group identifies/agrees together, to avoid reinventing wheels.
Then, as ‘phase 2’ of this initial toolkit design workshop, 10 representatives of 7 Companies and 2 people from 2 trade associations joined a 2-hour virtual meeting on 23rd June. Here, the participants provided feedback on the overall added value of a toolkit and how best to orientate it, whilst commenting on the usefulness and feasibility of tools in the same domains explored in the Bari event.
An interactive Miro board was created, to incorporate all specific comments collected over both workshops. Specific remarks and perspectives were grouped against each proposed domain (e.g. Legal Framework Tools) for this toolkit, along with potential tools (e.g. data sharing principles) suggested to sit within each domain.
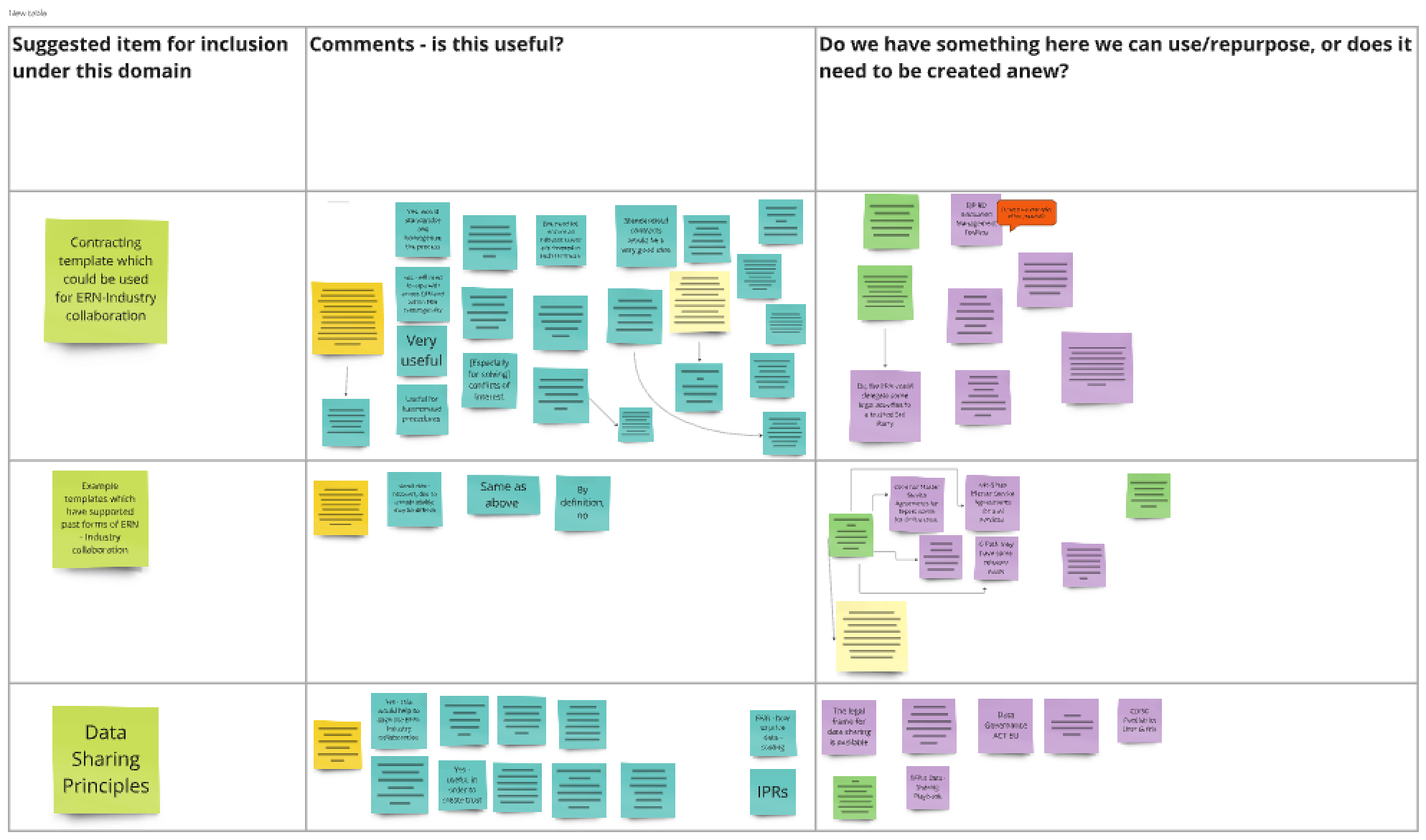
It also captured examples of existing assets or resources which participants wished to highlight to Together4RD, as possible tools to include in order to maximise use of what is already available and avoid reinventing wheels.
This Miro board formed the basis for structuring this Toolkit – both envisaging what a future, mature Toolkit might look like, and what this current version should encompass.
Both workshops raised a number of fundamental, cross-cutting points concerning the nature and added value of this toolkit, and realistic steps needed to create and then evolve the resource. The workshop participants also identified additional strategic issues of relevance here, in terms of enhancing ERN-Industry collaborations beyond a toolkit.
Overarching Comments to guide the Toolkit development
The Bari workshop, in particular, highlighted the fact that the importance of the BoMS Statement -and therefore, by extension, the necessity to try to change it – remains a controversial topic, with people sometimes holding polar opposite views here. To those who would remark that the two Statements really only reflect the views of a minority of MS who advocated for particular caution in public-private partnerships, the group was reminded that Statements have to be adopted by consensus. We should look closely at the 2019 Statement and focus on what it does allow, regardless of any decisions as to whether to seek for a more supportive wording.
We need to think about whether we are creating tools to fill gaps and needs quite unique to the ERN ecosystem, OR if instead we are simply signposting to a community that does not know much about PPP and may lack experience. Again, this was particularly a message from the Bari workshop. This is important, as if we go solely for the former, it will be a relatively contained toolkit. If the latter, we risk straying into a situation where we are trying to ‘teach’ researchers (and it would largely be researchers, as opposed to Industry, probably) about how to do research well, how to work with Industry, how to think about regulatory issues, etc. All agreed it is important we do not try to take on that larger task and seek to focus as far as possible on what is unique for the ERN situation and balance it with key materials to support public-private partnerships or PPPs (NB: the guiding question is ‘how to do PPPs’, not anything and everything to do with ‘research’).
Both workshops entered into some discussion on whom the toolkit should really be aimed at – will it be more useful for Industry or for ERNs? Both workshops saw a benefit for both sets of stakeholders, in the end, albeit different benefits for each. For instance, the Industry workshop on the whole suggested that perhaps ERNs could benefit from a more concrete setting-out of expected roles and responsibilities, timelines, and steps to collaboration, whilst acknowledging that the general Industry awareness of ERNs and what they could offer is relatively poor, and they need to better understand mechanisms for working with the Networks and what the added value could be compared to ‘business as usual’. It is important to note that even representatives of the more research-mature ERNs felt they would benefit significantly from a toolkit. Both workshops also highlighted the fact that ERNs really are very heterogenous and have different needs – this is often mentioned, but should not be underestimated.
This would ideally be an iterative toolkit. In the Industry workshop, creating the toolkit was likened to ‘paving a way to a road we want to walk’ – some participants cautioned that we should not seek to be too premature here, as building capacity to do these types of collaborations well will take time. It is sensible to start with the ‘low-hanging fruit’ e.g. if a legal template or model contract is deemed beneficial, it’s unlikely this can be created very quickly. And unsurprisingly, both workshops strongly supported our mantra of not reinventing wheels with this exercise. Again, it is important to maintain balance between building capacity for ERN-Industry interactions, on the one hand, and generally upskilling academics/clinicians to do research here. It is good that we have some resources which can support with the latter, like the EJP Innovation Management Toolbox. The T4RD Toolbox should also try to reflect, in this signposting, the types of activity Together4RD is particularly concerned with, avoiding duplication: for example, when it comes to actually planning and performing clinical trials, c4c-s has developed tools such as Service Level Agreements and Master Agreements which (although not publicly accessible) but could be highlighted in connection with those specific sorts of activity.
Participants in the Industry workshop, in particular, emphasised the fundamental importance of agreeing an appropriate and specific research question for ERN-Industry collaboration. There was a general feeling there that idea generation, at least focusing down to a really specific activity, could benefit from more ERN direction – “right now, it seems that although there is huge potential there, all the key people in each ERN have in mind different research questions for different purposes.” This arguably reinforces the need for tools supporting the kind of collaboration that could be entered into. Nonetheless, it is important to emphasise that the pilot experiences of generating research questions have, by their very nature, not been typical examples of the way in which projects might usually – or might in future- be proposed. Here, stakeholders in both the ERN and Industry communities were keen to work together on something, to test the notion of ERN-Industry collaboration, and one could argue that that spirit of collaboration was the key driver, ahead of the generation of a really concrete research question – here, the partners were chosen before the research question, in a way, and that wouldn’t necessarily be the case moving forwards.
Both workshops emphasised that when considering tools relating to the pilots, e.g. the ‘lessons learned’ report, that we recognise that these ARE pilots, and they may not work how we want them to work. Related to this, it may be important to convey the message that in these early forays, choosing a small project that can achieve a specific goal, is preferable to a vast project. It is imperative that we keep expectations realistic, at least at first. Furthermore, these ‘scoping’ and ‘developing research questions’ domains need to acknowledge that just because a pilot learnings report explains how something worked or did not work for a given ERN, it is important to remember that ERNs are not one size fits all. Again, they are very heterogenous, thus learning lessons may not be applicable across the board.
There were some questions, especially in the Industry workshop, around the possibility of structuring some of these tools according to different types of collaboration that could be envisaged. For instance, this toolkit could somehow distinguish between two broad types of collaborations – those with a defined beginning and end and a very specific research question and accompanying protocol; and then, on the other hand, those collaborations seeking to fundamentally impact how care is delivered to patients, such as reducing time to diagnosis by implementing algorithms, which will likely require ongoing care and maintenance. These are fundamentally different kinds of partnerships and will require different kinds of legal structures, for instance. Building on this, it was further proposed that rather than tying this work too closely to the first pilots, perhaps this toolkit (or future versions) could return to the beginning a bit and think instead of all the different types of collaboration we could envisage. Both workshops proposed revisiting the table of possible activities for collaboration, included with our Position Statement. Participants to the Industry workshop suggested three obvious categories for activities could be research, healthcare delivery, and education. Each of these will likely involve different structures and different roles and responsibilities, and different steps, e.g. in terms of how you contract, which could allow future versions of this toolkit to be more practical. If a collaboration is really in the ‘research’ space, how can research be done – is it an ERN/ERNs working with Industry to explore unanswered research questions and see what can be answered using the data currently available, or creating something new, to address new questions? If the collaboration is more about education, what areas would be in focus: would it be about organising webinars, and if so, to whom would they be targeted (patients, healthcare professionals, etc?).
Notwithstanding future directions for the toolkit, it was acknowledged that there will be core functions and core practical steps that need to be taken in all activities; therefore, the toolkit as it stands was created with some more general recommendations on roles and responsibilities and timelines, with the possibility for others to build from there.
The eventual content of this Toolkit
In view of the comments received across all consultation activities in 2024, the tools included below fall under three headings:
- Background knowledge – ERNs, Industry, and the Opportunity
- Conceptualising and firming-up a collaborative idea or research question or project
- Practical knowledge transfer – initiating and delivering a well-developed research collaboration
The current resource does not include tools pertaining to ‘the legal framework’, as it was felt that identifying or creating resources here would require much more discussion. Furthermore, this was quite a divisive point, with participants in both workshops adopting very different stances on the feasibility of developing templates for contracts or agreeing common contracting clauses. In both workshops, some supported the concept of trying to develop more standardised contracts (to deal with the fact that different centres have very different contracting styles). Or if a standardised contract is not doable, perhaps clauses that all need to use could be identified. The concept of a ‘playbook’ was also raised, with some standardisation in contracting templates for each category of activity we could foresee. However, all of this would require further work.
It is important to emphasise once more the complementarity of this toolkit to the broader Innovation Management Toolbox or IMT (originating under the EJP RD and maintained under ERDERA, the European Rare Disease Research Alliance). This contains myriad tools which can support translational research per se, which, although not created specifically for ERNs, nonetheless obviously covers many key topics and can provide support to ERN research. Tools in the IMT focus on key areas such as robust project management (e.g. the EATRIS Research Management Manual), understanding regulatory requirements, ethical and legal issues, etc.
And of course, as this Together4RD Toolkit is not intended to be exhaustive, and does not address every topic emerging from the 2024 consultations, it should be used in connection with other key resources, beyond the IMT, which address these priorities. For instance, the need for robust data management was unsurprisingly highlighted during the Together4RD consultations, and although there is no dedicated ‘data’ section in this toolkit, resources like the 2024 Data Sharing Playbook are available. The importance of engaging and involving patients and other people with lived experience in rare disease research cannot be underestimated, and again, a number of tools exist to support this, such as the ‘Short guide on patient partnerships in rare disease research projects’ generated through the EJP RD in 2020, and the Rare 2030 Recommendations (especially chapter 5 on ‘Patient Partnerships’).
Related Resources
In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceThe Playbook provides a practical, user-friendly guide to navigating the complexities of data sharing in IMI/IHI collaborative health research projects, outlining key concepts, roles, decision points, common challenges, and strategies to address legal, technical, and organisational obstacles. It encourages early planning, stakeholder engagement, and adoption of standardised best practices to accelerate data sharing and improve research efficiency across multi-partner consortia
View this resource Bookmark this resourceTool 1: The Importance of Public Private Partnerships in Rare Disease
This resource explains the importance of public-private partnerships or collaborations for the rare disease community, in the light of the needs of the rare disease field and the current climate around research and innovation.
Tool 2: Examples of Initiatives which Foster Public-Private
Partnerships in Rare Disease and Complementary Areas
This resource presents examples of programmes and structures which facilitate public- private partnerships in rare disease or a complimentary area.
Tool 3: What are ERNs?
This Tool:
- Explains the origins of ERNs.
- Highlights key resources concerning the conceptualisation, set-up and operations of ERNs, including the legal documents on which they are based.
- Points to useful reports and recommendations concerned with analysing the achievements and added-value of ERNs to-date, which suggest where there might be room for improvement.
- Points to key resources showcasing the achievements of the ERNs, as a whole, as well as where to learn more about the achievements of specific ERNs.
Tool 4: The advantages of ERNs as partners for research
This Tool illustrates how and why ERNs hold so much potential for research. It is based upon content prepared for the Together4RD Position Statement of 2023, and has been updated to include the latest statistics and development connected with ERNs’ research potential.
Tool 5: Needs and priorities for Industry – and what does Industry need in a collaboration with ERNs?
This is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs.
Related Resources
This resource explains the importance of public-private partnerships or collaborations for the rare disease community, in the light of the needs of the rare disease field and the current climate around research and innovation
View this resource Bookmark this resourceThis resource presents examples of programmes and structures which facilitate public private partnerships in rare disease or a complimentary area.
View this resource Bookmark this resourceThis tool explains the origins of ERNs and highlights key resources on their conceptualisation, set-up and operations, including the legal documents on which they are based. It also points to reports and recommendations that analyse the achievements and added value of ERNs to date, indicating where there may be room for improvement, and to key resources showcasing the achievements of ERNs overall as well as where to learn more about the achievements of specific ERNs.
View this resource Bookmark this resourceThis Tool illustrates how and why ERNs hold so much potential for research. It is based upon content prepared for the Together4RD Position Statement of 2023, and has been updated to include the latest statistics and development connected with ERNs’ research potential
View this resource Bookmark this resourceThis Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceOne barrier to ERN-Industry collaborations, especially for ERNs in fields with limited R&D and Industry engagement to date, is a difficulty in envisaging:
- The type of activities that ERNs and Industry might engage in, beyond the major programmes like IHI which support public-private
partnerships broadly - The mechanics of enabling collaborations – how can ERNs work with Industry when they are not legal entities?
This section of the toolkit has been designed to support the initiation of projects between ERNs and Industry, by firstly
- summarising what the first 3 official Together4RD pilots, initiated in 2023, planned to do
- highlighting specific examples of public-private collaborations in the rare and highly specialised conditions space, outside of these pilots (largely pre-dating the ERNs)
- proposing a range of activities, beyond the traditional clinical trial or more standard involvement in IHI projects, for instance, on which ERNs and industry could work together to generate added value.
Tool 6: Brief Summaries of the first Together4RD Pilots
The first pilots showcased by Together4RD came about from an open call launched by the Together4RD secretariat in the summer of 2022. All ERNs were invited to submit an expression of interest through a survey, which asked Networks to outline the nature of the proposed collaboration with Industry, the added-value of the activity suggested, readiness to begin, how many ERN centres might need to be involved, any existing assets, data, or infrastructure the pilot might build upon (and who owns these), etc.
This survey has been further developed to form Tool 11, a List of Questions people could ask themselves when considering a collaboration between ERNs and Industry
The Industry sponsors of Together4RD were also encouraged to submit the same survey, to outline their proposals for a pilot. The Together4RD Secretariat initiated discussions with all parties submitting a proposal, wherever possible matchmaking ERN ideas with an appropriate Industry partner, along with other actors deemed essential to the project proposals. These discussions led to the identification of three pilots deemed feasible for launch in 2023.
The negotiations to evolve the initial ideas for a collaborative project have been, in all three cases, quite lengthy, unsurprisingly as these were the first pilots in this space. Important learning lessons have been captured, to streamline this process in future.
Tool 7: Case Studies – examples of previous or ongoing public- private collaborations in the Rare Disease space
Case studies for public-private collaborations in the Rare Disease space – beyond the T4RD Pilots
In addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects.
A frequently-heard criticism of the two Statements on ERN-Industry interaction issued by the Board of Member States of ERNs, was that not only are collaborations between ERNs and companies essential to enable ERNs to fulfil their research potential, but that seeking to avoid any interaction here is illogical and frankly a retrograde step for the field. For many years, experts argued, networks or other types of consortia or groups of non-industry actors, had been delivering successful projects and collaborations with industry, covering a wide range of activities. One of the first activities for Together4RD was to explore some of these prior examples of engagement and collaboration, and a set of case studies were included to the 2023 Position Statement on collaboration between European Reference Networks and industry, largely in the form of supplementary material (supplementary file 1). These case studies have been revised and updated and are included here as a tool to support ERNs and industry in considering what kind of projects might be beneficial for their communities.
Tool 8: Summary of areas or activities for potential ERN and Industry collaboration
Stakeholders sometimes struggle to consider the range of activities on which ERNs and Industry could collaborate, besides the more traditional engagement around clinical trials, or more recently, partnering with multiple companies through the European Federation of Pharmaceutical Industries and Associations (EFPIA), in a large project via the Innovative Medicines Initiative, for instance. This resource builds upon material prepared for the comprehensive Together4RD Position Statement, to present a table listing a broad range of potential projects and activities which might be well-suited to ERN and Industry collaboration.
Related Resources
The first Together4RD pilots resulted from an open call launched in summer 2022, inviting all ERNs to submit an expression of interest outlining proposed industry collaboration, added value, readiness, involved centres, and any existing assets, data or infrastructure to build upon.
View this resource Bookmark this resourceThe consultations and outreach activities undertaken by Together4RD over the course of 2024 highlighted certain issues or topics which, whilst ultimately not exactly fitting the brief for this Toolkit (in the sense of there beingexisting tools, or tools Together4RD could prepare alone, for a 2024/5 launch) they nonetheless deserve a mention here as they are very much connected to the overall mission of Together4RD.
View this resource Bookmark this resourceIn addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceStakeholders sometimes struggle to consider the range of activities on which ERNs and Industry could collaborate, besides the more traditional engagement around clinical trials, or more recently, partnering with multiple companies through the European Federation of Pharmaceutical Industries and Associations (EFPIA), in a large project via the Innovative Medicines Initiative, for instance. This resource builds upon material prepared for the comprehensive Together4RD Position Statement, to present a table listing a broad range of potential projects and activities which might be well-suited to ERN and Industry collaboration.
View this resource Bookmark this resourceTool 9: Report on the Experiences and Learnings from the first ERN-Industry pilots supported by Together4RD
In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report.
Tool 10: Key recommendations for both ERNs and industry from the experiences of the first ERN-Industry pilots
Based on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations.
Tool 11: Questions people should consider when approaching a new collaboration between ERNs and Industry
Related Resources
In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resourceThe consultations and outreach activities undertaken by Together4RD over the course of 2024 highlighted certain issues or topics which, whilst ultimately not exactly fitting the brief for this Toolkit (in the sense of there beingexisting tools, or tools Together4RD could prepare alone, for a 2024/5 launch) they nonetheless deserve a mention here as they are very much connected to the overall mission of Together4RD.
View this resource Bookmark this resourceThe consultations and outreach activities undertaken by Together4RD over the course of 2024 highlighted certain issues or topics which, whilst ultimately not exactly fitting the brief for this Toolkit (in the sense of there being existing tools, or tools Together4RD could prepare alone, for a 2024/5 launch) they nonetheless deserve a mention here as they are very much connected to the overall mission of Together4RD.
Defining ERN-Industry Interaction
The Together4RD Position Statement highlights the challenges of defining ERN Research as one of the factors which, historically, has limited ERN research. The Statement explains that “how to distinguish the achievements of a given ERN, collectively, from the day-to-day achievements of its component centres (and, at a still more granular level, of the individuals involved in that ERN)’ has been something of a challenge when generating performance indicators to showcase many different activities of an ERN”.
If we look at the latest document concerning the 19 core indicators issued by the ERN Continuous Monitoring and Quality Improvement System (ERN CMQS), an example Indicator each ERN must report on is ‘Number of accepted peer-reviewed publications in scientific journals regarding disease groups within the ERN and which acknowledge the ERN’. The Definition for this is as follows: “The total number of unique peer-review publications that have been accepted in scientific journals regarding disease-groups within the ERN and within the specified time period. Publications should be PubMed accredited scientific journals and involve as major contributors at least two Health Care Providers from two different Member States within the ERN, and which include an explicit acknowledgement
of the ERN such as “This work is generated within the European Reference Network for…” or “This work is supported by the European Reference Network for….””
Such specificity is clearly necessary to distinguish what individual experts would do even if the ERN did not exist from what may be deemed a collective ERN effort. It may be, therefore, that confusion over what constitutes research activity of an ERN has actually hampered research, or certainly hampered the reporting of this. And just as research-related indicators have been somewhat overlooked to-date, there is rather a lack of criteria for measuring and capturing ERN-Industry interaction. This issue is raised very often, when Together4RD events speak of past, present and future ERN-Industry engagement – how, precisely, does one define ERN-Industry engagement? As the Networks are not legal entities, a contract from ERN X with Company Y could not be a criterion. As more ERN- Industry projects and collaborations are launched, and the added-value of such activities becomes increasingly recognised by all quarters, some form of agreement on the basic parameters for counting or measuring this activity will be necessary. For instance:
- is the perception of the ERN coordinator that an activity is an ERN-Industry collaboration sufficient to make it ‘count’ and distinguish it from activity of a single investigator?
- should there be some stipulation that an interaction needs to involve more than one HCP of a given ERN, even if contracting is focused on one HCP with that one company?
- should there be a requirement that the project is discussed and approved in a working group of the ERN or that investigators from other ERN centres besides the HCP taking on the contracting are named in the project proposal or any MoU or similar?
- should there be a requirement for the project to be highlighted and agreed as an ERN activity in the Exec Board meetings or General Assembly?
Together4RD believes that although such requirements may be raised in the course of its activities, a formal definition and agreement should probably be the task of the official ERN Monitoring activity highlighted above, with the eventual criteria agreed by all 24 ERNs
It is important, however, that any criteria agreed in future should not be so strict as to actually hamper ERN-Industry collaboration.
Lack of opportunities for ERN and Industry Engagement to be initiated
One of the major points of consensus across the consultation activities which supported creation of this Toolkit, was the acknowledgment that there is a lack of opportunity for ERNs and Industry to really understand what each other is doing – for this reason, Together4RD initiated very important discussions around ‘a forum for information exchange’ (or perhaps a forum for collaboration).
It will be extremely important for such a forum, or fora, to be supported, in order to initiate more projects and collaborations between ERNs and Industry, beyond the kinds of large consortia projects funded via IHI, for instance. Although representatives of Companies occupying strategic positions, e.g. in EFPIA or EUCOPE, tend to be quite familiar with ERNs and their potential, most Industry representatives have generally been unable to participate in ERN meetings or workshops. And smaller biotech companies, lacking a strong European footprint, are likely completely unaware of what ERNs can offer. Together4RD proposed a range of options for a forum to help foster research collaborations, ranging from more general events enabling people from all ERNs and Companies to connect, to much more specific and bespoke activities.
What might a Forum for Exchange or Collaboration look like?
Pan-ERN research Conferences
In the early years of ERNs, the European Commission organised 4 large in-person ERN conferences. Should these resume, it should be possible to invite Industry representatives to join the general event and thus hear about the latest successes across ERNs, collectively. Alternatively, some level of awareness raising could be achieved by involving Industry in other key research conferences dedicated to showcasing ERNs and their achievements/ interests.
Pan ERN-Industry strategy forum
Moving a step beyond simply inviting Industry to conferences as observers, a dedicated space could be created for representatives of all ERNs and Companies to come together via an ‘ERN-Industry strategy forum’. ERN Coordinators and/or their research leads could meet once or twice a year with Industry representatives and patient representatives,
to strategically discuss a subject of mutual interest, from a general (i.e. cross-disease) perspective, of interest to many or all Networks. The model of the EURORDIS RoundTable of Companies could be viewed as a starting point.
ERN-Specific Industry research forum
A more dedicated forum could be envisaged, to host more specific and involved discussions between Industry and individual ERNs. (NB: this would not necessarily need to be mutually exclusive with the previous ideas – one could envisage a shared event at first, which then focuses down and splinters into ERN-specific sessions, each involving representatives of the Companies most interested in/active in the area with which that ERN is concerned.) Such a forum could take place back-to-back with other meetings, such as the twice-annual ERN Coordinators’ meetings, in which all ERNs participate; however, only coordinators and project managers attend, which could be a drawback. Alternatively, such meetings could take
place back-to-back with the annual General Assembly each ERN organises. This would be convenient, from the ERN experts’ perspective, and all the key HCPs and researchers would, in theory, be present, which is an advantage; naturally, there would be parts of the GA itself which would need to be closed off.
If scheduling back-to-back does not make good sense, and people were willing to make space for additional meetings in their calendars, one could envisage standalone meetings convened purely for this purpose.
One low-hanging fruit, potentially, is to arrange meetings as part of major disease-oriented conferences (e.g. those run by scientific societies), at which ERNs might routinely bring a booth and a contingent. The feasibility and usefulness here depends on how many of the ERN researchers would actually be present at these conferences. A formal meeting should perhaps be scheduled, as opposed to merely informal drop-ins at the ERN booth. But even the latter would be a step in the right direction.
Wherever they take place, these kind of strategic meetings could perhaps take some inspiration from the events organised by the ACCELERATE initiative in the paediatric cancer field, and the Multi-Stakeholder meetings run by the IMI project c4c. (Different types of agenda could be envisaged for communities in which there is less research activity and therefore less of a need to prioritise compounds or approaches.)
ERN-specific research matchmaking events
An even more hands-on version of a forum to foster ERN-Industry dialogue would be to envisage cross ERN or ERN-specific research matchmaking events, along the lines of the French ‘Proof of Concept’ club for rare diseases. Here, a collective of researchers from an ERN could actually pitch their research proposals to Industry colleagues, and a trusted third party would facilitate appraisals and support the development of ERN-based research emerging from the POC meetings.
Together4RD has already advocated for a forum for exchange of information, along the lines of some of the options outlined above. However, it will be important for ERNs and Industry to take the initiative -either under the aegis of an initiative like Together4RD or otherwise- to realise some of these opportunities, to help initiate future proposals and maintain the momentum created by Together4RD.
Thinking to the future – what role could/should a trusted third party play in supporting ERN-Industry collaborations?
During the consultations of 2024, and indeed beyond, the question of whether or not a trusted 3rd party (which would be a legal entity) would be useful in supporting ERN-Industry collaborations in future was quite divisive. Some view this as very useful, in fact essential, in order to scale-up the volume and scope of future ERN and Industry engagements.
“The third party role in a PPP is critical, both conceptually and in practice”
“A third party could provide experts in negotiation, PPPs, contracting, IP etc. This would be very helpful”
Others however see potential to slow things down and overcomplicate collaborations.
“No – this could block or slow down effective collaboration”
“Better to have a lean coordination without ‘heavy’ infrastructures”
The consultations highlighted a range of existing organisations that could potentially take on such a role, ranging from translational research infrastructures used to working in the rare disease space, to paediatric infrastructures and services, to small consultancies, foundations and CROs. Some suggested it would be wise to look to a single dedicated third party, or cluster thereof, to specialise in supporting ERN and Industry collaborations in future, in order to build critical mass of knowledge and experience. And indeed, a further suggestion was to create or appoint something quite new, such as a team established at European level for this very purpose, which also included legal specialists, clinicians, and patient representatives. Several experts also noted that it would be useful to explore more precisely how ERN-Industry collaborations might be delivered through the intermediary of Medical/Scientific Societies – especially where an educational activity is envisaged. To this end, it would be useful to know which ERNs consider themselves to be working with Industry through Medical Societies (or feel this is a good structure for the future).
In summary, however, for the purposes of this Toolkit, it would be premature to attempt to provide any strong stance on the desirability and feasibility of this, nor propose suitable third parties to play an intermediary role. Together4RD recommends that such discussions are prioritised in the future by the research structures most closely connected to the ERNs themselves, utilising the resources in this Toolkit (and especially, the ‘lessons learned’ from the Together4RD pilots).
Related Resources
C4C Expert Advice service gives you fast and efficient access to over 400 clinical, methodology, and patient and public involvement experts.
Their up-to-date and in-depth insights can provide value at any stage of paediatric drug development but are especially useful to improve study design.
We provide end-to-end support, resulting in high-quality, independent advice reports that can be used in regulatory discussions on PIPs (paediatric investigation plans) and PSPs (paediatric study plans )
Obtain multidisciplinary insights from a single request and a single contract.
A tailored team of experts is assembled for each request.
Improve patient recruitment and retention through making a study more patient-centric based on the insights of children, young people and families.
The challenges posed by rare diseases to patients, families, researchers, clinicians, healthcare systems, policymakers, regulators, the private sector, and more, are well documented.
-
- Although individually rare, the sheer number of conditions classed as rare (often estimated as 6-8000) result in a significant population directly affected by a rare disease of one kind or another (equating to approximately 1 in 18)
- Rare diseases are typically complex, multisystemic conditions, around 75% of which are genetically inherited.
- The presentation, severity and outlook differ dramatically – some conditions do not manifest until adulthood, and patients are able to live a relatively normal life with few restrictions. Approximately half present in childhood and around a third of paediatric patients will die before their 5th birthday.
- Only 5-6% of all conditions classed as rare have any dedicated treatment, and those which do tend to be clustered around one of a limited number of therapeutic
areas (60% of orphan designations during the period 2010-2020 were for oncology, alimentary tract and metabolism, and musculosketal and nervous system disorders.)1 Furthermore, many treatments address symptoms only, and are not curative or transformative. - There is growing evidence that rare diseases tend to impact negatively on all aspects of daily life. The 2017 pan-rare-disease survey ‘juggling care and daily life’, led by the RareBarometer initiative under EURORDIS, demonstrated that 7 in 10 rare disease patients or carers reduced or stopped professional activity, 8 in 10 have difficulty with daily care activities, and were 3 times more likely to be depressed than the general population.2 The most recent RareBarometer survey illustrates the strong link between rare disease and disability – 8 in 10 people living with a rare disease report a disability, and the majority of these consider their disability3 invisible, and poorly addressed.4
- All of these challenges result in significant inequalities for patients and their families.
The Together4RD position statement on collaboration between European reference networks and industry (2023) summarises5 how Europe, in particular, has sought to address these challenges (much of the remainder of this introductory section comes from this report).
Key policy documents were issued in 2008 (the Commission Communication on Rare Diseases: Europe’s challenges [COM(2008) 679 final]6) and 2009 (the Council Recommendation on an action in the field of rare diseases (2009/C 151/02)7). These landmark policies built upon the regulatory incentives engendered by the 2000 orphan drug Regulation8 to call for national action alongside key European efforts to advance diagnostics, treatment, care, research and social support for rare diseases. Much has been achieved in the following decade and a half; for instance
- 26 of the current EU MS have adopted a national plan or strategy for rare diseases, compared to only 4 in 2008. This does not mean all countries have kept these policies live and updated, of course, but it is an important achievement nonetheless
- 24 European Reference Networks were launched in early 2017, for rare and specialised diseases
- Transnational research initiatives dedicated at the pan-disease level (such as the successive E-Rare projects, the European Joint Programme for Rare Disease research (2019-2024), the ERNs’ own research project ERICA, and most recently the European Rare Disease Research Alliance, ERDERA) increased the opportunities for collaboration
- Umbrella patient organisations such as EURORDIS (Rare Diseases Europe) grew
to become a key stakeholder in rare disease projects, whilst also establishing, supporting and networking national alliances of rare disease patient organisations - Orphanet (the global database for rare diseases) evolved to encompass a large suite of tools to complement its nosology and disease encyclopaedia
- Diagnostics initiatives at the pan-RD level were launched and sustained, such as RD-Connect, Solve-RD, Screen4Care, etc., along with the expansion of the Undiagnosed Diseases Network to include an International focus.
- Over 260 marketing authorisations granted for orphan products since 2000 and over 3000 with orphan designations.9
However, notwithstanding these achievements at both European and national level, the day-to-day reality for too many people living with a rare disease has sadly changed little. Major unmet needs remain, which can only be addressed through a seismic shift in the way in which research, care and social support are organised, in Europe and beyond. In recent years, much attention has been focused on where the RD field should go next – how can we stimulate new R&D for the thousands of conditions without any treatment options (and indeed any fundamental research foundation), whilst also ensuring that therapies developed for conditions benefiting from a relatively strong research interest hitherto deliver meaningful and transformational change?
The Together4RD Position Statement further noted that “Rare Disease research, in particular, needs to operate within a supportive Research and Innovation ecosystem”. A ‘supportive’ Research and Innovation ecosystem, able to tackle the needs of rare diseases, must have several components.
Related Resources
Together4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resource
The RD-Connect Registry & Biobank Finder is an online directory of existing rare disease databases, registries and biobanks.
The RD-Connect Registry & Biobank Finder lets researchers find the rare disease patient registries and biobanks that store data on their rare disease of interest. The system provides databases’ contact data and the numbers of registered cases for each disease in the registry/biobank, regularly updated by the database curators.
Users can search the directory by disease name and its synonyms, ORPHA- or OMIM-codes and other keywords, such as the country or registry manager. The system also provides access to documents such as databases’ study protocols, case report forms, informed consent templates and data access agreements.
Legislation which fosters and incentivises research
The foundation for any rich Research and Innovation ecosystem must be the existence
of robust policies to incentivise R&D. Therefore, the importance of the efforts to revise
the Orphan Drug Regulation (EC 141/2000) and EU Paediatric Regulation, cannot be understated. In 2017, a 10-year evaluation report on the EU Paediatric Regulation was published. This report concluded that the Regulation had provided positive results overall in terms of paediatric product development, but that development for rare paediatric diseases, which is in many cases equally supported through the Orphan Regulation, often failed to materialise. Following this report, the European Commission announced a joint evaluation of the Paediatric and Orphan Regulations, which provided an assessment of the strengths and weaknesses of the two Regulations. On this groundswell of activity, a European Expert Group on Orphan Drug Incentives10 was established and in 2021 published a comprehensive and much-needed report on ‘How to address the unmet needs of rare disease patients by transforming the European OMP landscape, complete with recommendations and policy proposals.11 A key conclusion was that to force meaningful progress in the therapeutic landscape for rare diseases requires the optimisation, application and integration of many elements, initiatives, and actors. The eventual changes to the EU General Pharmaceutical Legislation will be finally determined in 2025; however, the impact of proposed revisions has, over the past couple of years, dominated much of the debate around the future of rare disease research in Europe.12
Acknowledgement of rare disease as a priority area for research – at national, European and global level
Next, a supportive Research and Innovation ecosystem entails a broader acceptance by European bodies and national-level stakeholders that rare disease matters, in a world of competing health threats and priorities and increasing financial pressures. The Rare 2030 foresight study issued an ambitious set of recommendations in 202113, intended to guide Europe towards the future scenarios deemed most favourable by its expert panel of over 250 individuals (and indeed thousands of stakeholders, globally, through Rare 2030’s wider consultation sand surveys). The key message espoused across the individual chapters of recommendations is that there is an urgent need for a new European policy framework for rare diseases. Since the end of the Rare 2030 Foresight Study, many stakeholders, galvanised by the efforts of EURORDIS, in particular, have advocated for a renewed European commitment to rare disease, evidenced perhaps through a new Commission Communication or Council Recommendation, but most likely via an EU Action Plan.
However, as R&D for rare disease rests upon the engagement of the private sector, and companies working in rare disease tend to have a global outreach and footprint, it is important to accompany any European prioritisation of rare disease research with a strong and growing global acknowledgement of the major unmet needs facing the 300+ million people living with these conditions worldwide. Here too, there has indeed been an increase in momentum at the global level. Back in 2011 the pan-disease International Rare Disease Research Consortium (IRDiRC) was established, to unite researchers with research funders. The new European Rare Disease Research Alliance, ERDERA, funded through Horizon Europe, is forging closer links with IRDiRC and will more broadly pursue global collaborations in rare disease research. In the areas of healthcare, policy and general awareness-raising, important developments have been seen over the past couple of years at the global level. Rare Diseases were mentioned for the first time in a United Nations (UN) Declaration on Universal Health Coverage, in September 2019. This was followed by the adoption of a UN Resolution on Rare Disease14 in late 2021. Recognising that rare diseases are the source of major inequalities in health and wellbeing globally, and that those dealing with these conditions face major inequities, the WHO signed a MoU with Rare Disease International (RDI) in 2021, to scope a Global Network for Rare Disease.15 In 2025, RDI has launched a campaign for a World Health Assembly Resolution on Rare Disease.16 All of these developments are important, to stimulate more focus on research and innovation for rare conditions across the globe, building awareness and prioritisation in regions and countries traditionally lacking rare disease policies.
The opportunity to build effective multistakeholder collaborations
It has long been recognised that addressing the many gaps and challenges in rare diseases entails a truly cross-sector and cross-disciplinary approach. Years of public and private research investment has achieved much, but, as the Rare2030 foresight study concluded, much remain to be done, and all stakeholders must play a part, pooling resources and skills:
“The rare disease community aspires to a research, development and delivery ecosystem for rare disease therapies in Europe in which efforts at the local, regional, national and international levels remain concerted for success. This ecosystem must be co-designed by both public and private sectors.”17
This means that any and all prospective research in rare conditions must be patient-centred, and should involve patients as early as possible, from the design of the project or activity, as partners, not merely as subjects.18 It means that the networks and structures created to build a critical mass of experts in the clinical and research domains relevant to rare disease (most obviously the ERNs, but also considering for instance national-level networks for rare conditions, the landscape of paediatric trial hubs established by conect4children, and more) must be supported to perform world-leading research (which, in the case of perhaps the most important category here, the ERNs, has traditionally NOT happened as yet, for many reasons).19 It means that funders, policymakers, regulators, HTA bodies, payers, and all the other actors necessary to:
- stimulate R&D in rare diseas.
- build new knowledge to apply in the clinical sphere.
- understand and address the social and holistic needs of people with rare disease;
- and develop new products and bring these to the people who need them.
… must collaborate in a concerted effort, spanning national boundaries, and even continental lines, to leverage advances in all areas that must be addressed if we are to leave no-one behind in rare disease and rare cancer.
A key stakeholder in this landscape is, and must remain, industry (encompassing both the pharmaceutical and devices sectors).
Again, one of the core recommendations from Rare 2030 under the chapter ‘Innovative and Needs-Led Research and Development’ was that “Long-term multinational public- private research partnerships should be enhanced”: because notwithstanding the value of academic and patient-led research into rare disease, the reality is that developing new therapies to address the significant remaining unmet needs requires the commitment of the private sector.
Related Resources
Together4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceWhen thinking about the broader context of public-private collaborations, beyond rare disease, there are increasing challenges, not least the concerning trend of a declining pace for R&D in Europe compared with other world regions. Whereas 41% of R&D investments across the board were centred on Europe in 2001, this has now dropped to 31%.20 The 2024 Draghi report on ‘The Future of European Competitiveness’ highlighted declining EU competitiveness across several key areas21 calling for stakeholders to “boost the attractiveness of the EU for conducting clinical trials and to expedite access to markets for novel medicines.” (p31). And a recent EUCOPE (EU Committee of Pharmaceutical Entrepreneurs) report22 highlights the fact that although Europe remains popular for early-stage investment, later stage clinical investments are continuing to decline, as the EU continues to lose ground to the US and China. It is imperative that Europe regains a competitive edge, especially in terms of research and innovation for rare disease, given the major unmet needs. To build more, and more fruitful, public private collaborations in rare disease, requires action of several fronts.
- Leveraging developments in the wider research space, beyond rare diseases, to continue to innovate in areas such as data, AI, personalised medicine, new technologies, trial design, and more.
- Ensuring more, and more diverse, concrete opportunities for the public and private sector to work together, both on large-scale initiatives of the kind funded via the Innovative Medicines Initiative and supported by the Rare Disease Moonshot, for instance, but also smaller scale projects and activities within specific disease communities or spanning therapy areas (see Tool 2).
- The advantages of working with the pharmaceutical industry, in particular, must be recognised by policymakers and funders, and in some quarters, perceptions on the value of collaborating with industry need to be addressed. As noted by the Together4RD Position Statement, although there can be, and have been, examples of poor conduct, and sometimes standards fall, the messaging must become more positive, more openly supportive.23
- Concrete and dedicated support for those wishing to take the step of forging collaborative activities with companies. When experts or centres or networks are not used to building connections with industry, the realities of what this might entail.
are not always well-understood, which can deter people from entering into such collaborations at all, or else jeopardise initial attempts to build a co-creative project. (This is one of the gaps this Together4RD Toolkit is intended to address)
Some of these essential steps will be more challenging than others. Some require resources, others a significant mindset change. But it is important that the field focuses efforts in these directions, as the bottom line is that building more public-private collaborations IS essential, since private sector involvement generally remains a prerequisite for successful drug development in the rare disease domain.24 There is very much a sense that the conditions without treatments, and indeed without a strong basic science footing, are the ‘higher-hanging’ fruit – developing therapies here will be difficult. Moving into an unstudied rare condition, which likely has a very small patient population, can means significant risks for companies – not only is there the scientific challenge of developing a products that would make a difference, but uncertainty about the regulatory processes and likelihood of a product making it to patients in jurisdictions like the EU, with all its heterogeneity around access, can be a deterrent that the traditional incentives for orphan product developers struggle to overcome. “Investing in PPPs helps organizations and stakeholders to share the risks of innovation in high unmet need areas, the cost of infrastructures, and the work required to acquire relevant scientific expertise with large datasets that translate discoveries into treatments.”25
The expertise drug development companies can bring, around clinical trial execution, regulatory pathways, data, and much more, coupled with their access to financial resources, is a vital combination. However, the process of advertising for, selecting, and launching Together4RD pilot projects to explore how ERNs and industry can work together, have illustrated relatively entrenched perceptions and misconceptions from the non-industry research community around the needs and expectations of the private sector. Besides providing support and tools to optimise collaborations, therefore, it is important that researchers in both industry and the public sector become better acquainted with each other’s realities and modus operandi. There are several useful resources to help the public sector in this respect (see Tool 5 ‘Needs and Priorities for Industry – and what does Industry Need from a Collaboration with ERNs?’)
Related Resources
This resource presents examples of programmes and structures which facilitate public private partnerships in rare disease or a complimentary area.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceIn addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceThe Innovative Medicines Initiative was set up in 2008 as a public-private partnership between the European Commission (public funding) and the European pharmaceutical industry (private funding, represented by EFPIA, the European Federation of Pharmaceutical Industries and Associations). The goal was to improve the medicines’ development process and make it more efficient, and to ensure that patients will have faster access to better and safer medicines. The first phase of IMI covered the period 2008-14, before evolving into IMI2 which spanned 2014-2020. The total budget of IMI 2 was EUR 3.276 billion. Of this, EUR 1.638 billion (half the budget) was pledged from Horizon 2020, whilst EFPIA companies committed EUR 1.425 billion to the programme (up to EUR 213 million could come from other organisations that wished to contribute to IMI initiatives as Associated Partners, for specific projects).
Across IMI 1 and 2, almost 200 projects were funded, dealing with a broad range of conditions. Some of these were particularly relevant for rare diseases, including:
- conect4children (see below)
- ARDAT project (looking at Advanced Therapy Medicinal products or ATMPs, which often target rare conditions)
- Screen4Care (exploring newborn screening for rare conditions, and how to foster earlier diagnosis from health record data)
- STOPFOP, which was seeking a cure for Fibrodysplasia ossificans progressiva (FOP)
- U-PEARL, dedicated to better trial design, specifically exploring platform trials, in four focal areas, one of which was the rare condition neurofibromatosis (including types NF1, NF2 and Schwannomatosis)
At the end of 2021, the IMI became the Innovative Health Initiative (IHI). This programme will last until 2027. The core principles remained the same, but the change in name reflected the recognition that different sectors need to be engaged in addressing life-sciences challenges and that “future breakthroughs in medical science will involve cross-sectoral discoveries, such as medical device / drug combinations or diagnostics based on artificial intelligence.”1 To reflect this broader scope, the private partners now include EFPIA, COCIR, Vaccines Europe, EuropaBio, and MedTech Europe. The total budget for IHI, for the period 2021-2027 is €2.4 billion. €1.2 billion comes from Horizon Europe; €1 billion will come from the IHI industry partners; and €200 million will come from other life science industries or associations that decide to contribute to IHI as contributing partners.
IHI has already supported rare disease-related projects, specifically Realise-D and PaLaDIn, with further rare-disease-related calls expected to follow.
For general resources on IMI and IHI, see below:
- Booklet providing an overview of the IMI
- Short video introducing IMI
- Blog on the IMI and its value
- IMI to IHI
- IMI post relating to rare disease public-private collaborations
A deeper exploration of IMI and IHI projects fostering public-private partnerships in rare disease
conect4children (c4c)
c4c is an IMI2 project (2018-2024, with extension to 2025) establishing a European network and streamlined ecosystem for clinical trials in paediatric diseases. It involves 36 academic partners, 10 industry partners from EFPIA, and an additional 500 affiliated partners.
As so many paediatric diseases are also rare diseases, c4c’s processes and tools to support better, more efficient and more successful clinical trials in children and young people also address broader rare disease needs. Besides developing tools to accelerate study start-up and address the pain points in initiating multinational paediatric trials, c4c included strands of work focusing on key topics such as education, training, PPIE and data standardisation. The achievements and resources of c4c, the public-private partnership, can be found on the project website in particular Connect4Children Achievements
Useful videos: see What is conect4children? and We are proud to conect4children! – The Movie

In 2023, c4c launched a dedicated legal entity, c4c-Stichting..For details of the c4c-S legal entity, see Connect4Children For a 1-page overview on what the c4c-Stichting can offer to ERNs, specifically, see here.
Screen4Care
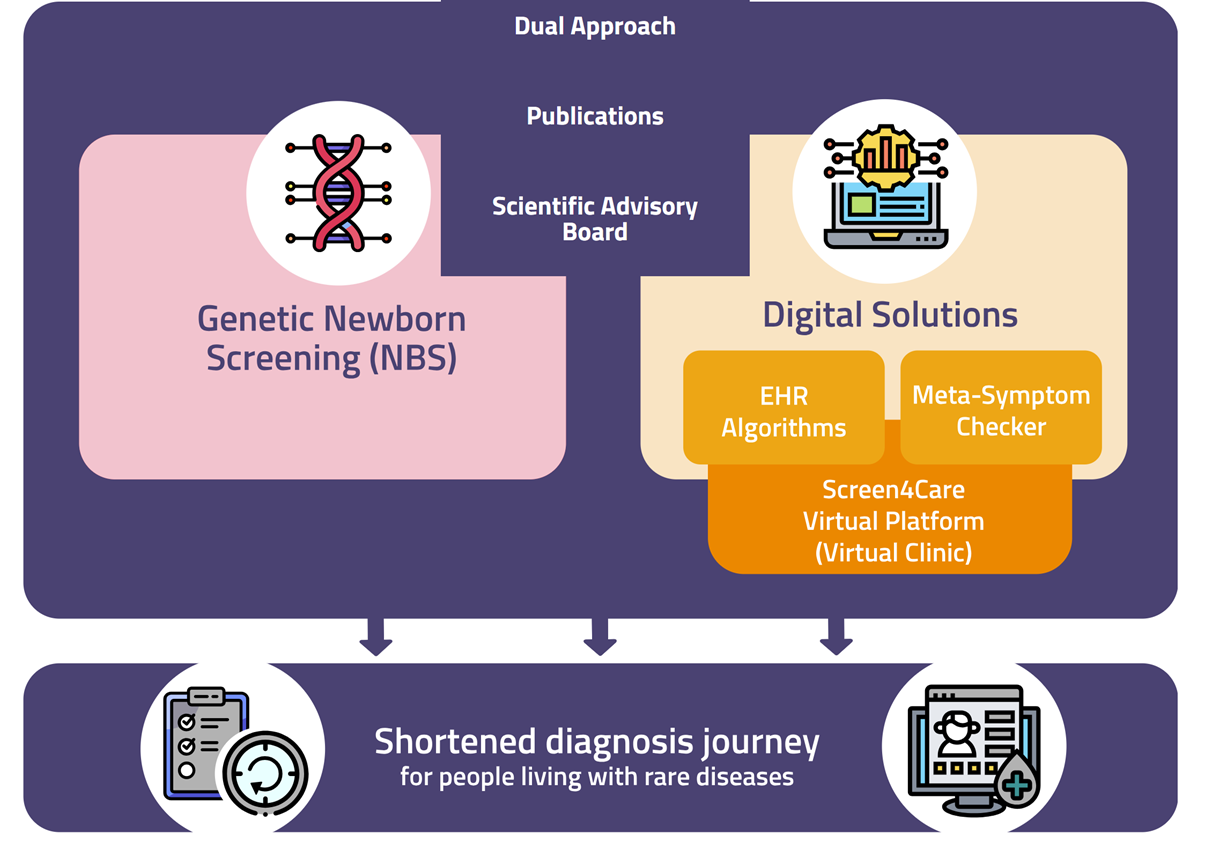
Screen4Care is a €25 million IHI initiative which launched in late 2021. It has two broad and interconnected pillars (see the Screen4Care visual, below):
- genetic newborn screening (exploring the use of genetic testing and related advanced genomic technologies); and
- AI-based tools to bring accurate diagnoses to patients, earlier, via predictive algorithms leveraging the Screen4Care federated data machine learning environment, and algorithms embedded in Electronic Health Record (EHR) systems that will flag patients at risk for rare diseases based on the data in their EHR.)
It is a five year project involving 37 partners from 14 countries. For more details, see the Screen4Care website and publications here and here.
Realise-D
Realise-D stands for ‘CompRehensive mEthodological Approach to cLinical trIalS in (ultra-) rarE Diseases’. This 5-year Realise-D public-private partnership began in January 2025, with an overall budget of €17 million. The goal is to optimise and accelerate the development of treatments for rare and ultra-rare conditions, by bringing together 40 partners representing stakeholders from many different groups (clinicians, methodologists, pharmaceutical industry researchers, representatives of patient organisations, regulatory agencies and HTA bodies) to develop cutting-edge operational and methodological tools and resources to dramatically advance treatment evaluation. The Realise-D project has a particular focus on ultra rare conditions and plans to create easy-to-use playbooks and digital tools for planning and running clinical trials.
PaLaDIn
This 4 year project began in 2024, with an overall budget of over €19 million. PaLaDIn is developing a state-of-the-art platform dubbed the ‘Interactium’ to drive innovative, real-world data collection from patients with rare diseases. The project focuses on rare neuromuscular diseases (NMDs), specifically Duchenne Muscular Dystrophy (DMD) and facioscapulohumeral muscular dystrophy (FSHD). The Interactium is expected to be able to integrate data from diverse sources, including neuromuscular registries, patient- reported outcome/experience measures (PROMs and PREMs), as well as digital outcome measures from wearable devices, all of which will be co-created with patients. The project is coordinated by a patient organisation and the partners include experts in NMDs, patient advocacy and data science. They hope that their results will not only improve the lives of people with NMDs, but will prove useful to other rare disease communities around the world facing similar challenges.
Related Resources
conect4children Stichting (c4c-S) is a non-profit, pan-European organisation that supports paediatric clinical research by providing expert advice and trial support services, including feasibility assessments and site identification, for ERNs and other stakeholders. Building on a successful public–private partnership, it mobilises a large network of experts and research-ready sites to improve the efficiency and quality of paediatric trials across Europe.
View this resource Bookmark this resourceThe Rare Disease Moonshot was launched in 2022, to bring together a coalition of partners able to accelerate scientific discovery and drug development in rare and paediatric diseases for which currently there is no therapeutic option. This is important, as the majority of rare conditions (approximately 95%) have no dedicated treatment, despite years of investment and research, and there has long been a question of how to shed much needed light and attention on these so-called neglected conditions (which not abandoning research in disease areas which have perhaps seen significant R&D but still lack satisfactory therapies and medicines).
The Moonshot coalition is informal, involving the CriticalPath Institute (C-Path), the European Infrastructure for Translational Medicine(EATRIS), the European Clinical Research Infrastructure Network (ECRIN), the Biobanking and Biomolecular Resources Research Infrastructure – European Research Infrastructure Consortium(BBMRI-ERIC), the European Federation of Pharmaceutical Industries and Associations (EFPIA), the European Confederation of Pharmaceutical Entrepreneurs (EUCOPE), EuropaBio, EURORDIS-Rare Diseases Europe, and the European Joint Programme for RareDiseases (EJP-RD/ERDERA).
These partners set out to both accelerate innovative research for rare conditions in Europe (for instance by developing novel trial designs, enhancing data infrastructure and trial networks, and defining specific approaches for ultra rare diseases), and ensure patients with rare and paediatric disease can access the latest innovations. The ‘USP’ of this approach is its multistakeholder ethos; in particular, the Moonshot partners extol the advantages of leveraging public-private partnerships to help pool resources and solve problems more quickly. Key Resources from the Rare Disease Moonshot Three key topics were selected for multistakeholder collaboration, and new sets of recommendations have been created for each. Although not specific to ERNs, these sets of recommendations are clearly very relevant to the goal of this Toolkit, namely advancing public-private collaboration between ERNs and Industry.
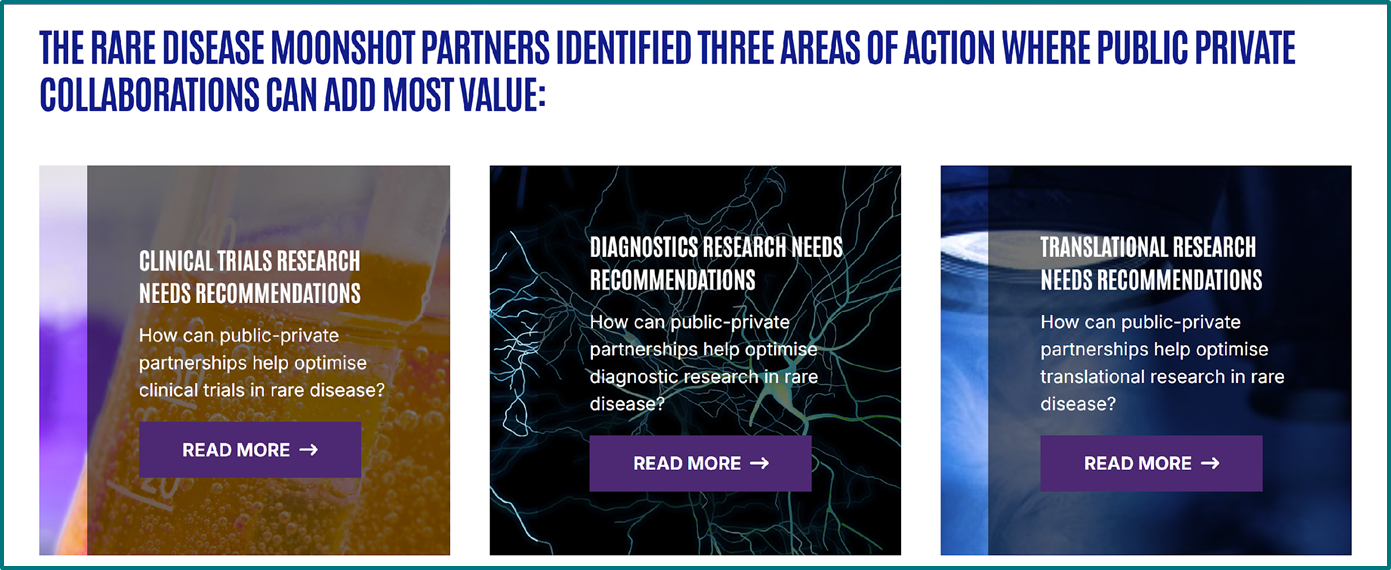
Key Resources from the Rare Disease Moonshot
Three key topics were selected for multistakeholder collaboration, and new sets of recommendations have been created for each. Although not specific to ERNs, these sets of recommendations are clearly very relevant to the goal of this Toolkit, namely advancing public-private collaboration between ERNs and Industry.
These sets of recommendations are the fruits of months of broad consultations with stakeholders including
- patient representatives
- global pharma/biotech companies
- small innovative enterprises
- academic translational research experts
- biobanking, non-profit clinical and fundamental research communities
- non-profit PPPs.
Rare Disease Moonshot Recommendations:
- How can public-private partnerships help optimise clinical trials in rare disease?Recommendations generated by a group of experts led by C-Path and ECRIN. 33 stakeholders contributed to their development, through workshops and consultations. The recommendations address topics such as disease prevalence, patient access, data standards, and regulatory support.Clinical trial recommendations
- How can public-private partnerships help optimise diagnostic research in rare disease?Work began in June 2023, with a workshop that brought together 30 industry participants. The final recommendations are the results of months of teamwork between the RD Moonshot team and stakeholders including industry, the research community and patient advocacy groups. Further input came from a series of additional workshops with industry partners and discussions in the EURORDIS Round Table of Companies, which gathered more than 100 participants.Diagnosis recommendations
- How can public-private partnerships help optimise translational research in rare disease?Development of this resource began with a workshop in February 2023, bringing together 33 participants from a broad spectrum of sectors. The initial discussions underscored the importance of interdisciplinary approaches, research coordination, and enhancing the skills of different stakeholders. The recommendations were further elaborated and refined via additional workshops, online consultations, and direct feedback sessions, involving over 20 stakeholders.Translational research recommendations
For more on the mission of the Rare Disease Moonshot and why public-private partnerships are so important, see here.
See further on this publication here.
ERDERA launched in September 2024, with an estimated budget of €380 million to support activities up to 2031. The overall goal of this large initiative is to improve the lives of people living with a rare disease in Europe and beyond. Over 170 organisations are involved, across 36 countries, giving ERDERA a global footprint to complement the European. This is a Horizon Europe Partnership, in which the EU is expected to contribute approximately €150 million, with the rest of the funding coming from EU Members States, countries associated to Horizon Europe, and in-cash and in-kind contributions from public and private partners. ERDERA is, in many ways, a successor to the EJP-RD, as it seeks to ‘bring under one roof all knowledge, resources and services, boost clinical research and spur innovation’ at the pan- rare-disease level. It also builds heavily on other key research initiatives like ERICA (the ERN- focused research action) and the Horizon 2020-funded diagnostics project Solve-RD.
There are many streams of interconnected activity in ERDERA, but the 3 main missions may be summarised as follows:2
- To bring together, in one place, a range of services, resources and cross-disciplinary expertise, in order to bring added-value to rare disease research
- To boost clinical research by ensuing every patient wishing to participate in research is somehow findable, and can be enrolled in a suitable clinical study
- To increase innovation and EU competitiveness, whilst evolving a global ecosystem for rare disease capable of linking the national, regional, European and global levels
ERDERA’s activities are structured around four key pillars:
- Funding – including dedicated financial support for collaborative international research projects, clinical trials, and knowledge exchange and networking initiatives.
- Clinical Research Network – Encompassing all ERDERA’s in-house research activities, this network will enhance diagnostics and clinical trial readiness
- Support Services – This includes a Data Services Hub to facilitate global data collection, integration, analysis, and sharing at a global scale; an Expertise Services Hub to offer guidance on specific aspects of translational and clinical research; and an Acceleration Hub that collaborates with industry partners to advance the most promising research projects and technologies. Additionally, ERDERA will maintain a robust Education and Training program.
- International Alignment – Through existing and newly established National Mirror Groups, the partnership will ensure alignment between national and international rare disease research strategies, particularly in nations that are behind in developing and implementing national plans. ERDERA will also host the Scientific Secretariat of the International Rare Disease Research Consortium (IRDiRC), a unique global consortium co-established by the European Commission and US National Institutes of Health back in 2011.
The ERDERA consortium includes private sector companies, including UCB Biopharma SRL, AstraZeneca AB, and Pfizer Inc.3 ERDERA is expected to foster public-private projects and collaborations through, for instance, the funding activities and calls, and the Acceleration Hub, in particular.
The EJP RD launched in January 2019, involving 93 beneficiaries and 48 linked third parties, with a total budget of approximately €110 million (€55 million directly from the EC, supplemented with substantial national and in-kind contributions). The EJP RD sought to create resources, services and expertise to advance rare disease research at the cross- disease level, through workstreams centred on funding opportunities, data, training, and accelerating innovation. The main public-private focus here came from the ‘Rare Disease Research (RDR) Challenges Call’. Industry partners were invited to identify 4 challenges to form the topics of the call, and these were validated by EJP RD Partners. A total budget of € 1.5 million was anticipated, from the European Commission, to allow 4 projects to be funded. The idea was that an independent committee would review the proposals and the industry partners who identified each challenge would then join the successful consortium of applicants, bringing in-cash and in-kind support.
The topics/challenges were as follows:
- Development of a non-invasive tool for measuring rare disease patient mobility in daily living (Industry sponsor – Chiesi Farmaceutici S.p.A. (Italy), CSL Behring (Australia))
- Delivery system for intranasal administration of biological drugs to neonates (Industry sponsor -Chiesi Farmaceutici S.p.A. (Italy))
- Characterize Rare Bone Disorders (RBD) Mobility Challenges in Real World Setting (Industry sponsor – Ipsen)
- Pre-clinical assay to detect instability of microsatellite repeat expansions (Industry sponsor – LoQus23 Therapeutics)
An example of a funded project emerging from this scheme (related to the 1st challenge) is the Digital Tools 4 Rare Disease (DT4RD) project.
Find out more here on these challenges here.
The International Rare Disease Research Consortium, IRDiRC, was launched in 2011, initiated by the European Commission and the NIH. It initially had two major goals: to create 200 new therapies for rare diseases and enable diagnostics for most rare disease, both by
2020. However, given the early success in meeting these goals the consortium revised its objectives in 2017. A new overarching vision was agreed, for the period 2017-2027: ‘Enable all people living with a rare disease to receive an accurate diagnosis, care, and available therapy within one year of coming to medical attention’. To achieve its goals, IRDiRC has undertaken numerous dedicated actions to increase access to harmonized data and samples, enhance the molecular and clinical characterization of rare diseases, support translational, preclinical and clinical research, and streamline ethical and regulatory procedures.
IRDIRC is organised into 3 constituent committees (dedicated to funders, companies, and patient advocates respectively) and 3 scientific committees (Therapeutics, Diagnostics, and Interdisciplinary).
In terms of the opportunity for public private collaboration, companies can be members of IRDiRC, alongside public funders. Biotech, Pharma, MedTech and more can join, by investing more than 10 million USD over 5 years in rare disease research. Much of the work of IRDiRC
is shaped by its three committees, which identify gaps and key issues in RD research, to be addressed via Task Forces and Working Groups who produce guidelines, recommendations & resources. These structures often involve both public and private sector experts.
Find out more here.
Another public-private partnership of relevance to rare diseases is C-Path. This is a non- profit PPP launched in 2025 to accelerate the pace -and reduce the costs- of medical product development through creation of new data standards, measurement standards, and methods standards that support the scientific evaluation of safety & efficacy of new therapies. C-Path provides the legal, scientific, and regulatory infrastructure to generate a unique neutral collaborative environment for stakeholders in the drug development ecosystem. The Institute fosters public-private collaboration across both rare and non-rare conditions; however, an important -and RD-specific- infrastructure under C-Path is the “Rare Disease Cures Accelerator – Data and Analytics Platform,” where industry can share data into a centralised and standardised infrastructure to support & accelerate RD characterisation to accelerate dev. of therapies.
European Reference Networks (ERNs) are arguably the single most important innovations in health and research for rare diseases in Europe, if not globally.
- There are 24 ERNs, launched in 2017, established across broad rare disease groups such as rare liver diseases, rare eye disease, etc., or are dedicated to areas of highly specialised medicine such as paediatric transplantation
- ERNs are networks connecting EU/EEA centres of expertise in specialised healthcare fields necessitating a concentration of expertise
- At present, they bring together 1613 Healthcare Providers/centres/units, nested in 382 separate hospitals across all 27 EU Member States plus Norway
- The primary focus of ERNs is improving care, and the networks are officially coordinated under the European Commission Directorate General concerned with Health (DG SANTE). However, they have strong research responsibilities and priorities too, offering enormous potential
- ERNs are designed to be patient-centred, with patients embedded in the governance and in all activities – this is facilitated by the concept of ePAGs (European Patient Advocacy Groups). Today, there are over 300 ePAGs working with ERNs
- The Clinical Patient Management System (CPMS), a secure digital platform used by the ERNs, has enabled the virtual consultation of more than 4000 complex cases
- Over 95,000 patients have already been included in the dedicated new ERN registries
The first formal call for ERNs was launched back in 2016, representing over a decade of preparatory work by so-called ‘pilot’ ERNs.1 A significant amount of planning lay behind that milestone moment, driven by the European Expert Groups for Rare Disease (EUCERD and the Commission Expert Group on Rare Disease), Joint Actions (the EUCERD Joint Action and RD-ACTION, in particular) and, crucially, advocacy from patient organisations, most notably EURORDIS. A model of possible disease groupings was developed,2 to help avoid hundreds -or even thousands – of applications seeking to set-up ERNs in individual diseases or small, clinically distinct groups of diseases. RD-ACTION worked with the European rare disease community to help ensure that each community would rally behind only one application, to avoid competing proposals and try to ensure all rare diseases could be categorised under at
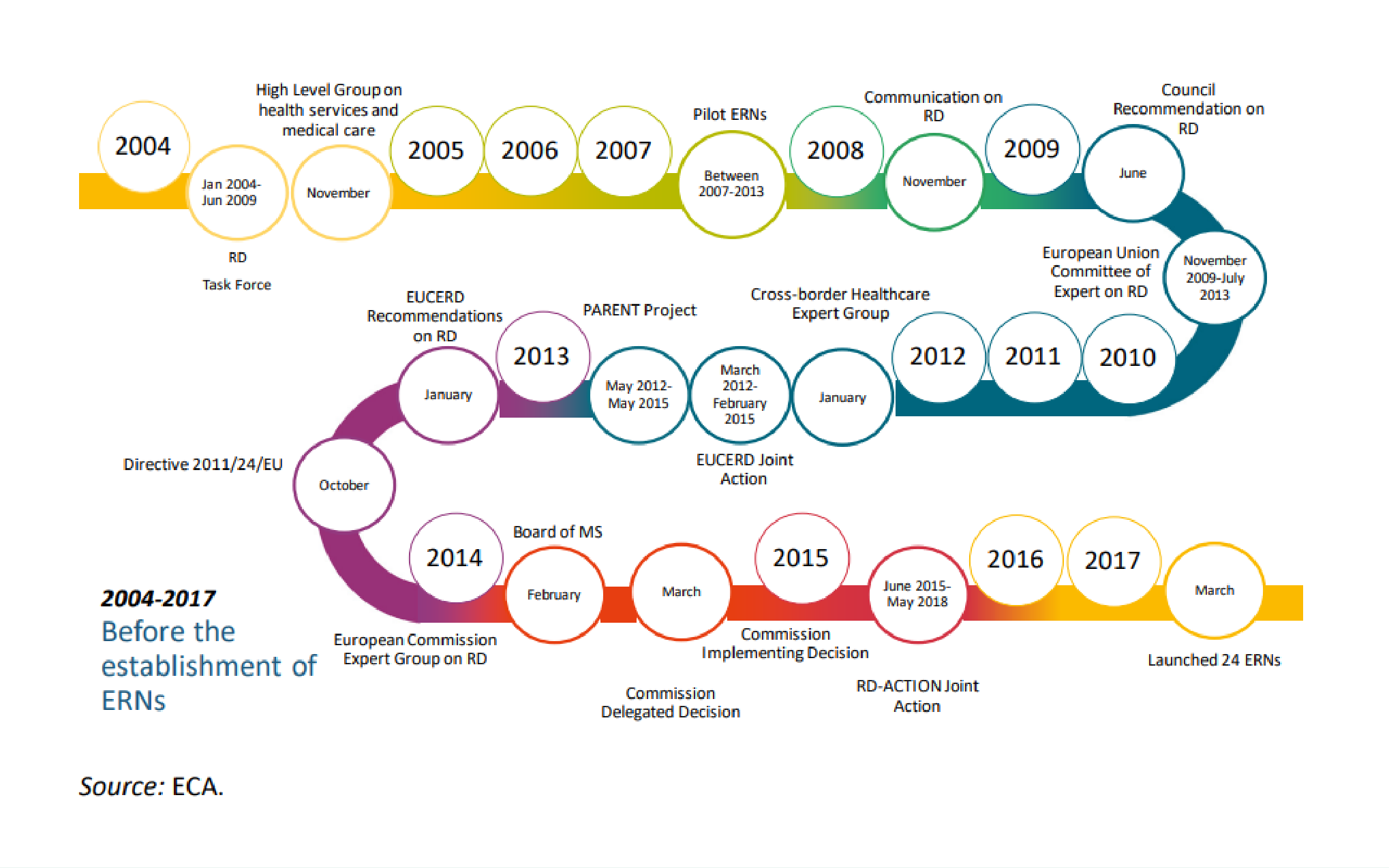
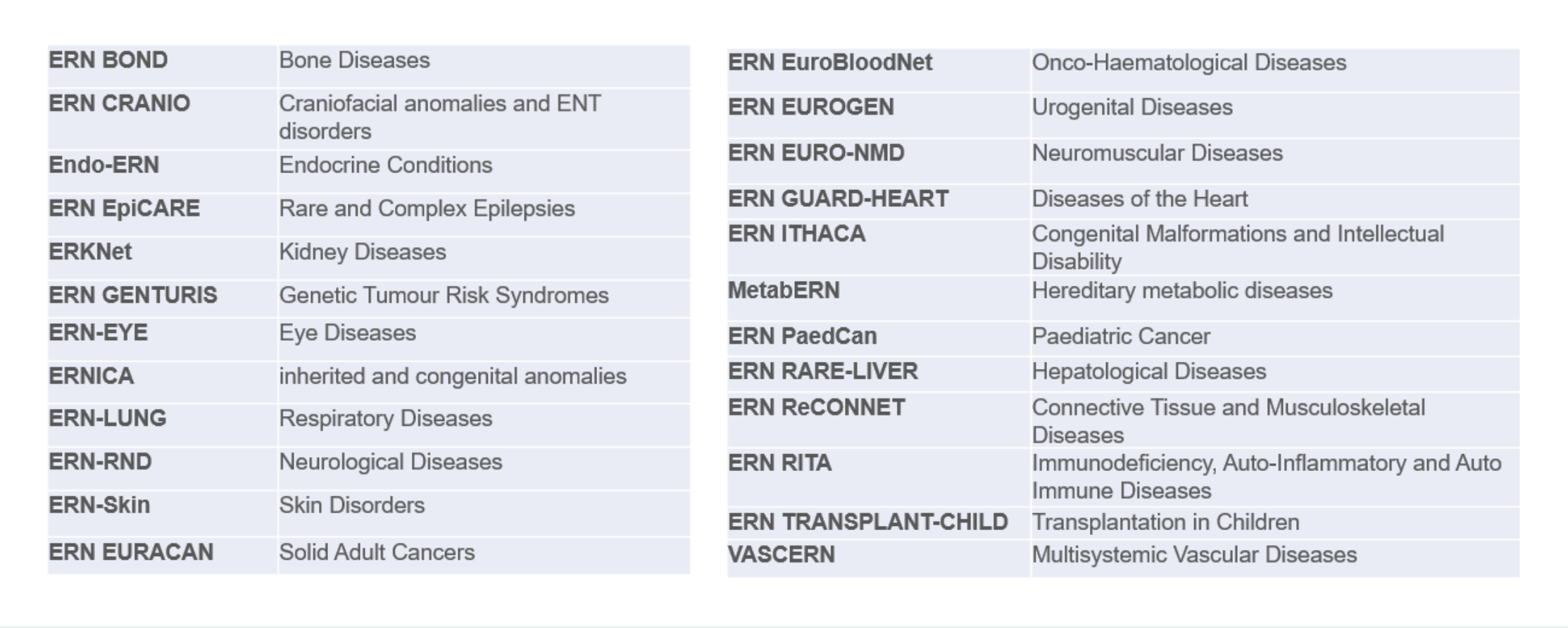
least one of these networks.3 The 24 Networks were officially launched in 2017.
In the end, their headings largely reflected the proposed model of disease grouping, with a few logical modifications to incorporate not only classifications of pathology but also areas of highly specialised healthcare which span across diseases. This was important, to achieve a central pillar of the ERN vision – collectively, across all ERNs, every rare disease should have a ‘home’. Cross-ERNs collaborations would also facilitate the need for multidisciplinary expertise when dealing with rare or ultra rare diseases. In this way, ERNs would strive to go beyond the networks created by past EU funding, via projects, which were dedicated to individual diseases or small groups of diseases, and would instead seek to improve diagnostics, treatment, research and care for all conditions under the rare disease umbrella. A further fundamental difference here was that ERNs are not projects – subject to 5-yearly evaluations, these Networks should be considerer permanent structures, revolutionising rare disease care and research across Europe.
At their launch, the 24 ERNs brought together over 900 specialist units in over 300 hospitals across 26 countries (25 EU MS plus Norway). These figures have increased in subsequent years (see ‘Getting to know the ERNs’ below), to include 1613 members, in total.
ERNs, as cross-border networks, have many substantial responsibilities, spanning the care and research domains. The tables below collate a non-exhaustive set of resources which:
- further explain the origins of the ERNs
- provide analysis/recommendations for their future functioning
- and illustrate the status quo across the Networks.
Origins of the ERNs – the concept, the criteria, the Legal Acts and the background
EUCERD Recommendations on Rare Disease European Reference Networks
Grey literature/ reports/ recommendations
Foundational recommendations on what ERNs should be and should do, adopted unanimously by the EU Committee of Experts on Rare Disease (EUCERD) on 31st January 2013. Incorporated and reflected past learnings from the field and formed the basis for the legislation which followed
https://www.rd-action.eu/eucerd/EUCERD_Recommendations/ern_recos.pdf
European Reference Networks for rare diseases: what is the conceptual framework?
Peer-Reviewed Publication
Héon-Klin, V. European Reference networks for rare diseases: what is the conceptual framework? Orphanet J Rare Dis 12, 137 (2017). https://doi.org/10.1186/s13023-017-0676-3 Presents a comprehensive overview of the story behind ERNs
Directive 2011/24/EU of the European Parliament and of the Council of 9 March 2011 on the application of patients’ rights in cross-border healthcare
EU legislation
This is the so-called ‘Cross-Border Healthcare Directive; the legislation on which the ERNs were established (Art.12)
https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32011L0024
COMMISSION DELEGATED DECISION of 10 March 2014 (2014/286/EU)
EU legislation
The Delegated and Implementing Acts (see below) form the key legal basis for the creation and governance of ERNs. The Delegated Decision sets out core criteria and conditions that ERNs, and healthcare providers wishing to join an ERN, must fulfil
COMMISSION IMPLEMENTING DECISION on 10th March 2014 (2014/287/EU)
EU legislation
Accompanying the Delegated Acts, above, this legislation set out the formal criteria for establishing and evaluating ERNs and their Members, and for facilitating the exchange of information and expertise on establishing and evaluating the Networks
EC Consumers Health Agriculture and Food Executive Agency. Rare diseases 2008-2016: EU-funded actions paving the way to the European reference networks
Grey literature/ reports/ recommendations
European Commission: Consumers, Health, Agriculture and Food Executive Agency, Rare diseases 2008-2016 – EU-funded actions paving the way to the European reference networks, Publications Office, 2018
Rare Disease European Reference Networks: Addendum to EUCERD Recommendations of January 2013
Grey literature/ reports/ recommendations
Addendum issued by the Commission Expert group on Rare Diseases (successor to the EUCERD) to supplement the original 2013 Recommendations. Provides further detail on 1) meaningful patient involvement and patient-centredness in ERNs; and 2) a proposed disease-grouping model to ensure comprehensive coverage of ERNs
Rare 2030 Knowledge Base Summary on ‘Access to Healthcare’
Grey literature/ reports/ recommendations
This was the eighth in a series of ‘knowledge base summaries’, essentially status-quo documents, published by the first foresight study for rare disease, Rare2030, in 2019. Section 3 summarises the background to ERNs, and lists some early achievements. It also includes a focus on the related concept of centres of expertise (section 2)
Overview Report on the State of the Art of Rare Disease Activities in Europe, 2018 Version
Grey literature/ reports/ recommendations
This large report summarises the status quo of a broad range of key topics related to rare disease, based on data and research collected in 2018. Section 5 is dedicated to the rise and early activities of ERNs and provides good background to the early years.
Analysis of the ERNs To-Date – Evaluations, Recommendations, Statements
Tumiene, Birute et al. “European Reference Networks: challenges and opportunities.” Journal of community genetics vol. 12,2 (2021): 217-229. doi:10.1007/s12687-021-00521-8
Journal article by many key people closely involved in ERNs. Analyses the ERN progress and vision comprehensively, and identifies challenges to the Networks fulfilling their potentialhttps://pubmed.ncbi.nlm.nih.gov/33733400/
Kole A, and Hedley, V,. Recommendations from the Rare 2030 Foresight Study: The future of rare diseases starts today (2021)
Full Recommendations published in 2021, emerging from the first foresight study for rare disease. Created through the input of over 250 experts from all stakeholder groups, these Recommendations cover a very broad range of topics, and include a section dedicated mainly to recommendations concerning ERNs (section 3 p.49 onwards). Useful for understanding how and where the RD community sees a need for ERN evolution and supporthttps://download2.eurordis.org/rare2030/Rare2030_recommendations.pdf
ERNs evaluation results report – Independent Evaluations of European Reference Networks and of Healthcare Providers
Official report published in 2024 and commissioned by the European Commission, to fulfil the legal requirement for ERNs and their member HCPs, to be evaluated every 5 years. The report presents a mix of self-evaluations, document reviews, ERN interviews, on-site HCP audits and stakeholder interviews. The results showed a high level of commitment of ERNs to their objectives, with a significant proportion (100% of ERNs and 89.7% of their members) achieving satisfactory results in the evaluation. The report shows areas of strength, as well as areas where improvements were recommended.https://health.ec.europa.eu/latest-updates/erns-evaluation-results-report-independent-evaluations-european-reference-networks-and-healthcare-2024-11-29_en
Recommendations to Achieve a Mature ERN System in 2030
Recommendations generated by EURORDIS, reflecting the perspectives of their member patient groups and individual ePAGs, on the vision for a mature ERN system – reflects what patients feel is needed for these Networks to fulfil their potentialhttps://download2.eurordis.org/documents/pdf/Our_vision_on_mature_ERNs.pdf
Hedley, V., Bolz-Johnson, M., Hernando, I. et al. Together4RD position statement on collaboration between European reference networks and industry. Orphanet J Rare Dis 18, 272 (2023). https://doi.org/10.1186/s13023-023-02853-9
Peer-reviewed Position Statement addressing many key issues: outlining the historical reasons for limited ERN and Industry collaboration; explaining the work of Together4RD to improve the status quo; presenting case studies, precedents and ways of working between public and private sectors; and presenting recommendations to advance collaborations.This Statement includes many publications relevant for specific topics such as virtual care practices in ERNs, examples of ERN approaches to establishing new registries, etc.https://doi.org/10.1186/s13023-023-02853-9
Statement of the ERN Board of Member States on Integration of the European Reference Networks to the healthcare systems of Member States.
Board of Member States Statement from 2019, proposing 5 ways in which ERNs need to be better integrated to national health systemshttps://health.ec.europa.eu/system/files/2019-07/integration_healthcaresystems_en_0.pdf
Statement of the ERN Board of Member States on European Reference Networks and industry.
The first Statement on this topic, issued in 2016.https://health.ec.europa.eu/document/download/1ea98fa6-10be-4a84-bb79-ba7678efc8bf_en?filename=2016_statement_industry_conflictofinterest_en.pdf
Updated Statement of the ERN Board of Member States on ERNs and industry.
This is an updated Statement from the Board of Member States, issued in June 2019https://health.ec.europa.eu/system/files/2020-03/statement_industry_conflictofinterest_en_0.pdf
Getting to know the Networks – the Status Quo
The official website of the ERNs under the European Commission contains a lot of information about the Networks as a whole, the role of the Board of Member States of ERNs (which is the main executive oversight body for the ERNs), links to important official documents, etc. It is also a good place to learn more about any single Network, through factsheets (see for example Figure 3) and links to the individual ERN websites. Several of the specific resources highlighted below can be found from this main page.
A very useful resource is a new report published by the European Commission:
in March 2025: “European Reference Networks: A success story for patients living with a rare disease”. This report presents the most recent stats on each ERN – detailing how many centres are engaged in ERNs at present. Following the initial call in 2016, which invited proposals for both the creation of ERNs and for constituent individual health care providers (HCPs) (including entire clinics, hospitals or specialised units within a larger institution), a second call was launched in 2019, with new members integrated in 2021.
Today, the 24 ERNs unite 1418 centres/units as full members, and an additional 195 members across two categories of formal ‘affiliation’ status (these are centres which do not fulfil all horizontal and disease-specific criteria established by the European Commission and ERNs themselves, respectively, but will enable every country to access the expertise of an ERN more readily). This gives a total of 1613 members, nested in 382 separate hospitals across all 27 EU Member States plus Norway.
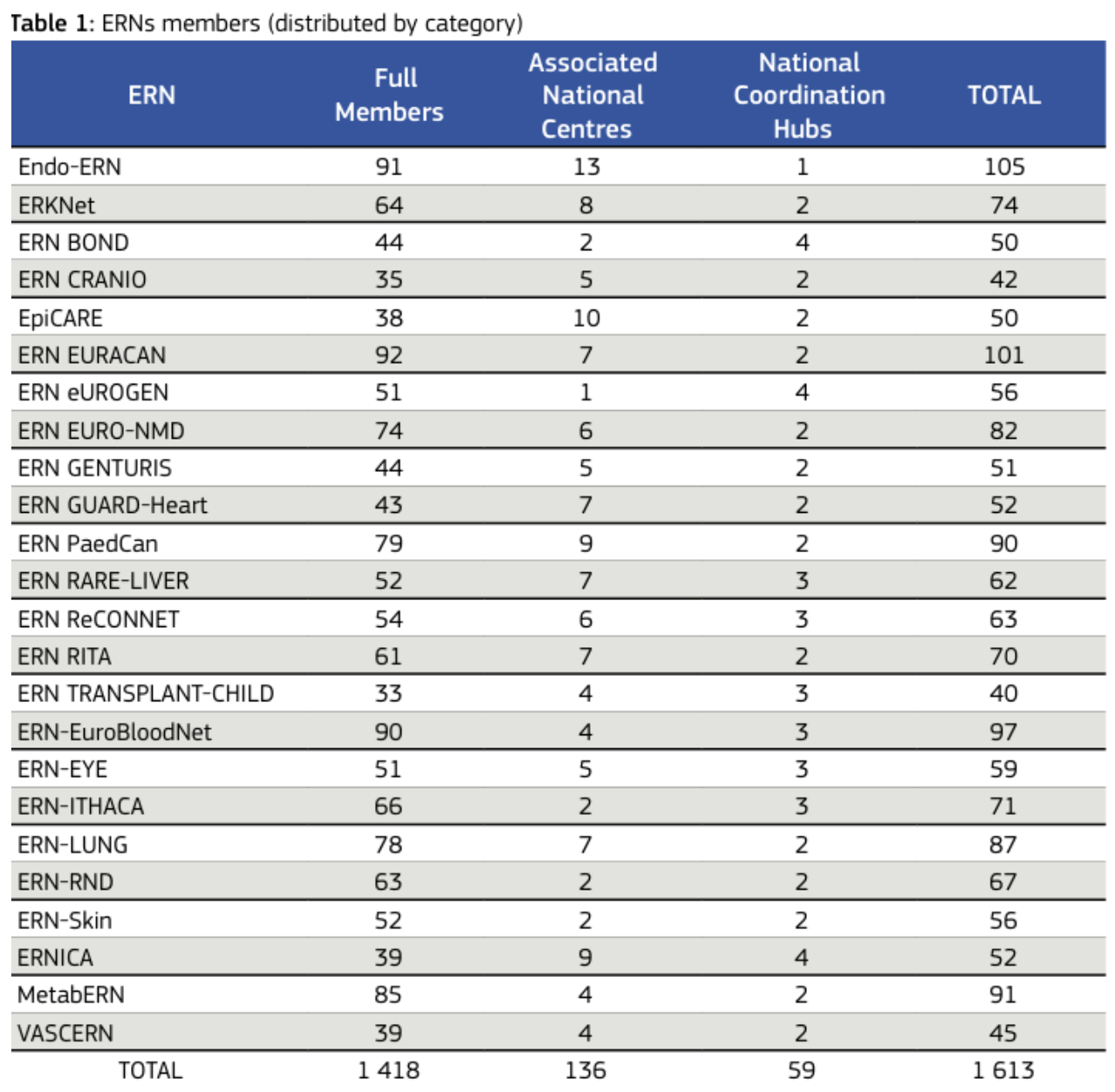
When compiling the information provided by each ERN, as summarised in this 2025 Report, several impressive statistics emerge; for instance:
- The networks range in size from 42 to 105 HCPs, with seven of them engaging over 80 HCPs each.
- Use of the CPMS for virtual consultations varies from a small number of consultations per ERN to over 500, with a total of over 4000 complex cases reviewed to-date.
- Over 170 clinical guidelines or clinical decision support tools have been written by the ERNs, collectively, a figure which, when adding-in guidelines co-authored with ERN HCPs or endorsed by the Networks, rises to over 590 resources.
- Over 95,000 patients are registered across the new ERN registries, based on the estimates provided here by each Network.
This 2025 report also presents case studies showcasing the most effective and innovative achievements of the Networks, for instance;
- activities in support of patients in Ukraine
- efforts to make medicines available to patients in times of supply shortages
- reactiveness under the Covid-19 pandemic.
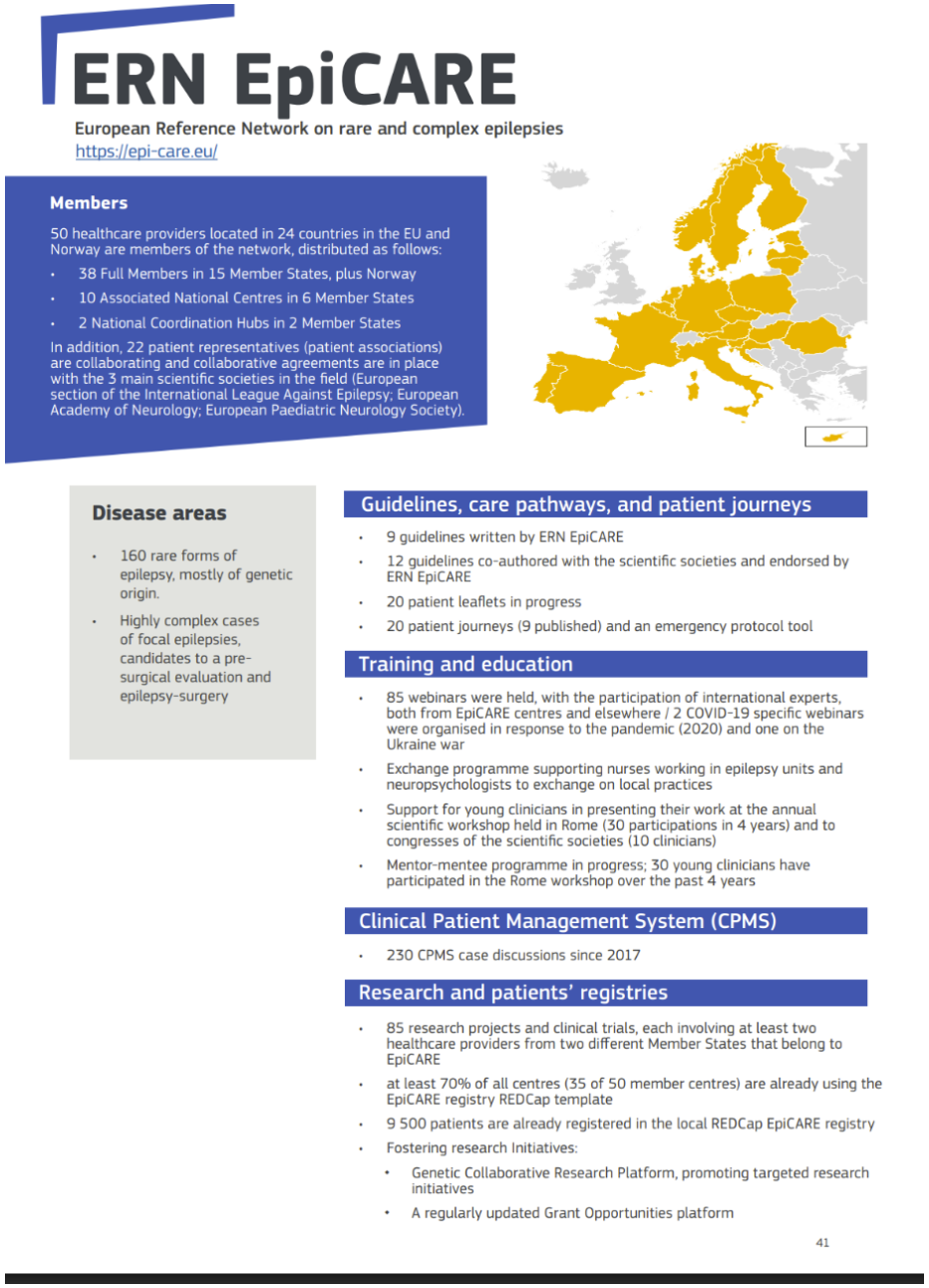
This 2025 report also presents case studies showcasing the most effective and innovative achievements of the Networks. Although only established in 2017, the ERNs have proven themselves highly agile and reactive in times of crisis:
- Only a few weeks after the onset of the COVID-19 pandemic, nearly all ERNs organised webinars during which experts provided concrete advice, to both patients with rare diseases and their treating physicians, on how to deal with drug suppliance/ shortage, drug interactions, risks in using -or not using- antivirus treatments, indications and safety related to vaccinations, and quality of life issues related to “stay-at-home” decisions. In partnership with their respective scientific societies they also produced several peer reviewed recommendations.
- Similarly, when Ukraine was invaded, the ERNs offered support to doctors working in the country or to refugees in EU countries. For instance, a dedicated website provided contact details for each of the 24 ERNs.
The resources highlighted in the table below (which include this recent European Commission report) are ERN-agnostic, and are intended to introduce the status quo at the cross-ERN level. The best way to learn about the achievements and what is happening in each individual Network is to visit their individual websites, which will link to publications, training materials, the registries established by each, and much more.
European Reference Networks – 2023 presentation booklet
An official brochure, updated in 2023, which provides a brief overview of every ERN
https://health.ec.europa.eu/publications/european-reference-networks-2023-presentation-booklet_en
Factsheets for individual ERNs
You can download a factsheet for each of the 24 ERNs explaining, for instance, a little about the conditions under that heading, who the coordinator is, what clinically-distinct subgroups the Network is composed of. See fig. 3
European Reference Networks: A success story for patients living with a rare disease
An official report published by the European Commission in March 2025, presenting the most recent stats on each ERN – detailing how many centres are engaged in ERNs at present, for instance. The report has a stats page for each Network, covering achievements in areas such as CPMS (virtual referrals), registration of patients, training & education materials, guidelines, and more. The report also presents patient case studies, showing how ERNs have made a difference, and includes particular highlights from across the ERNs as a whole, such as support for Ukraine, collaborations across multiple ERNs, achievements in creating Postgraduate degree programmes, etc.
A video on the ERNs
An official video created by the European Commission. This one is focused on explaining ERNs to patients and healthcare professionals
Websites for individual ERNs
This website provides direct links to the websites of each ERN. These sites provide a lot of information on the structure of the ERN, the governance, the centres who are members/associated partners, news & events, key resources, and much more
Downloadable zip-folder – List of Centres which are officially involved in each ERN
A means of searching for all centres which are formally part of any given ERN
Downloadable zip-folder – List of centres in each country which are formally involved with ERNs
A means of searching to see which centres in any given EU or EEA country are members of any ERN (and which one/ones they are part of)
Webinar – ERNs: a key EU infrastructure to partner for research activities, the why and the how
A webinar organised by Together4RD and the ERICA project (supporting ERN research), designed to introduce ERNs to anyone unfamiliar with them. A further goal is to bridge the knowledge gaps between ERNs and the pharmaceutical and biotech industries, fostering collaborations that can accelerate research and development in rare diseases, ultimately benefiting patients and advancing medical science
Deliverable from ERICA – Monitoring Report on ERN Registries (2024)
This report was created by the Work Package on Data Collection, Integration and Sharing, and was last updated in Q1 of 2024. It summarises the different approaches and progress of ERNs around their registries, including type of registry (centralised, federated or hybrid); approaches to managing consent; data dictionary sizes, and types of data elements collected; HCP participation in ERN registries; cumulative records across all ERNs; and more.
https://erica-rd.eu/wp-content/uploads/2024/11/ERICA_D2.5_02_24_NEW.pdf
Publication on ERNs’ support for Ukraine
A publication in The Lancet highlighting the role of the ERNs in responding to the crisis in Ukraine
https://www.thelancet.com/journals/lanepe/article/PIIS2666-7762(22)00160-0/fulltext
Related Resources
The resource explains that European Reference Networks (ERNs) are a major EU healthcare and research infrastructure that bring together clinical expertise, data and specialised resources across Europe to tackle rare and complex diseases and are valuable partners for collaborative research activities. It emphasises the untapped potential of ERNs to engage with the pharmaceutical and biotech sectors, advocating for greater awareness and public–private partnerships to accelerate rare disease research and development and benefit patients
View this resource Bookmark this resourceEuropean Reference Networks (ERNs) are often viewed as structures dedicated first and foremost to care – and indeed, they do have significant duties under the heading of ‘advancing care’ (e.g. supporting virtual case review, generating guidelines, supporting training activities). However, ERNs also have a formal mandate to contribute to research into rare diseases and highly specialised medicine. Although these research goals have perhaps been somewhat overshadowed to-date, this research mandate is clearly there, in the legislative acts on which ERNs are based: Annex I of the Delegated Decision (2014/287/EU)1 stipulates that one of the horizontal criteria (i.e. criteria which all members of any ERN should fulfil) is as follows:
“(5) To fulfil the requirement set out in point (iv) of Article 12(4)(a) of Directive 2011/24/EU (‘make a contribution to research’), the Networks must: (a) identify and fill research gaps; (b) promote collaborative research within the Network; (c) reinforce research and epidemiological surveillance, through setting up of shared registries”
Although some ERNs have embraced research goals from their launch, in one way or another -particularly those which emerged from communities which were already quite research-focused – it is probably fair to say that for most Networks, research per se has been less of a priority to-date.2 The Together4RD Position Statement explains in more details some of the reasons for this.3
An important step in enabling ERNs to reach their research potential, particularly when it comes to fostering collaborations with industry, is ensuring that the advantages and potential of ERNs as partners for research are understood and appreciated.
Related Resources
Together4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceERNs are arguably the single most important innovations in health and research for rare diseases in Europe, if not globally.
- There are 24 ERNs, launched in 2017, established across broad rare disease groups such as rare liver diseases, rare eye disease, etc., or are dedicated to areas of highly specialised medicine such as paediatric transplantation
- ERNs are networks connecting EU/EEA centres of expertise in specialised healthcare fields necessitating a concentration of expertise
- At present, they bring together 1613 Healthcare Providers/centres/units, nested in 382 separate hospitals across all 27 EU Member States plus Norway
- The primary focus of ERNs is improving care, and the networks are officially coordinated under the European Commission Directorate General concerned with Health (DG SANTE). However, they have strong research responsibilities and priorities too, offering enormous potential
- ERNs are designed to be patient-centred, with patients embedded in the governance and in all activities – this is facilitated by the concept of ePAGs (European Patient Advocacy Groups). Today, there are over 300 ePAGs working with ERNs
- The Clinical Patient Management System (CPMS), a secure digital platform used by the ERNs, has enabled the virtual consultation of more than 4000 complex cases
- Over 95,000 patients have already been included in the dedicated ERN registries
A number of fundamental advantages of ERNs for research are highlighted below (NB: these are based upon Part 2 of the aforementioned Position Statement from Together4RD, which itself incorporated and expanded upon conclusions from the first EMA and RD- ACTION workshop dedicated to ERN research.4 These earlier ideas have been supplemented here with additional and updated content.
ERNs are permanent infrastructures
For many years, EU projects dedicated to rare disease – funded both through the Framework Programmes and the 1st and 2nd Public Health Programmes, in particular – often made good progress in establishing networks:5 these were dedicated to a diverse range of rare conditions, sometimes quite specific diseases (such as McArdle Disease; Duchenne Muscular Dystrophy; Wolfram, Alstrom and Bardet-Biedl Syndromes; etc.) and other times focused on broader clusters such as intoxication-type metabolic diseases, rare anaemias, and paediatric cancers. These projects were often called ‘pilot networks’, once the concept of ERNs was born in the lead-up to the publication of the Cross-Border HealthCare Directive. They built consortia linking expert centres across Europe, and undertook crucial activities like establishing registries, developing guidelines, creating patient support materials, setting-up biobanks, developing educational resources, and much more. A major challenge, however, was finding routes to sustain these networked communities and, in particular, sustain their newly-created infrastructure and tools, after the funding period ended. This was not conducive to such communities developing into research-active networks or communities with which industry might partner. ERNs, therefore, have a major advantage here, in the sense that they are NOT projects, and are not temporary. DG SANTE committed to formally evaluating the ERNs and their constituent HealthCare Providers, or HCPs, every 5 years. The process and results of the first evaluation, initiated in late 2022 and concluded in 2023, can be viewed here6 – in a nutshell though, the first evaluation concluded that “the ERN ecosystem is functioning well, meaning they are delivering on highly specialist work for rare disease patients such as consultations for diagnosis and therapies, the production of clinical guidelines and specialised trainings”. All 24 ERNs obtained satisfactory results, meaning none were targeted to be disbanded (88% of their member HCPs also obtained satisfactory results7). Presuming the ERNs continue to be evaluated positively in future, they may be viewed as permanent structures, making them important stakeholders for partnerships in research of all kinds. These are not groups of experts united by individual projects, whose structures and resources are likely to fall into disuse once the funding period ends.
ERNs sit at the interface of the Research and Clinical Spheres
The Legal Acts upon which ERNs are based mandate that the Networks provide added- value across both the clinical and research domains. This is essential in rare diseases, here traditionally that line between care on the one hand and research on the other has, of necessity, been somewhat blurred (when 94-5% of the conditions lack any dedicated treatments, it is necessary for treating clinicians to generate knowledge ‘as they go along’ and apply lessons learned from any and all emerging research studies, in order to provide the best possible care). All HCPs participating in ERNs as full members should – assuming they fulfil the EC’s horizontal criterial for all centres wishing to participate as full members of an ERN – possess clinical expertise in at least some of the conditions underneath the grouping of that ERN, but should also be research-active. The proximity of research spaces and the clinic is a major strength of the ERN model, facilitating the generation and translation of knowledge and best practice.
ERNs are designed to ensure comprehensive disease (and specialised procedure) coverage
When applications for the first 24 ERNs were submitted, would-be coordinators were encouraged to establish their Networks based upon a list of suggested Thematic Groupings:8 this was to ensure that collectively, all rare disease would have a ‘home’ under at least one ERN. In actuality, many ERNs followed this suggested Groupings schema very closely, and consequently the vast majority of conditions classed as rare are covered by the 24 Networks created under the first call, along with several less disease-focused ERNs more dedicated to specialised procedures and areas of medicine in which a concentration of expertise is also of paramount importance (e.g. ERN-TransplantChild). (One notable missing area, which was included in the recommended list of ERN groupings back in 2016 but was not eventually included in any application, is rare gynaecological diseases – it is possible that Gyneco-Obstetrics, along with additional specialised procedures as opposed to pathologies per se, will be addressed in a future call for new ERNs). The fact that ERNs are founded upon this principle of inclusion of all rare diseases is a major benefit and holds real potential for research of the future.
The word ‘potential’ is important here. Some ERNs consciously commenced operations by focusing primarily on a subset of conditions under their wider headings. And even where ERNs are very much trying to map resources and knowledge on any and all conditions under that heading, the reality for many networks is that there is usually a ‘focal’ disease or group of diseases which has attracted a relatively large amount of research attention to-date, and/or is better understood and supported in terms of diagnosis and care. This is sometimes a condition or group of conditions which were the focus of successful proposals under past European Framework Programmes or Health Programme calls, which enabled networking to emerge relatively early. These sorts of conditions are sometimes amongst the more common of the rare diseases (e.g. Duchenne Muscular Dystrophy and Cystic Fibrosis would be good examples) but it must be noted that even these more active areas often still lack truly transformative, let alone curative, treatments. EURORDIS, in its ‘Recommendations to Achieve a Mature ERN System in 2030’9 highlights the need for a stronger focus on the conditions which are currently somewhat out of scope, or not receiving the requisite coverage.
Of course, the fact that neglected conditions which have never seen significant R&D attention are technically included under the combined scope of ERNs does not magically translate into knowledge and research effort. It will take time – and resources – to generate understanding of the less-well-studied rare diseases, and build a basis for research to thrive. But crucially, the expectation is there that each ERN will, in time and via a stepwise approach, come to tangibly support the diagnostics, treatment, care and research for all rare diseases under their heading.10 Therefore, the inherently egalitarian nature of the ERN model is, in itself, a strong step in the right direct of casting much-needed light on the many thousands of so-called neglected diseases which have traditionally lacked any research interest.
ERNs offer unique data generation/linkage and digital health opportunities
ERNs provide unprecedented opportunities to collect high quality, relevant, and interoperable data. The Networks are based upon centres which have demonstrable expertise in particular areas, but the Networking tools and platform which connect these well-established centres are being created -or at least delivered- anew. This offers exciting opportunities for the over 1600 member HCPs across Europe to subscribe to best practices around collecting and pooling precious rare disease data which can support the provision of highly specialised care and advance research. The Clinical Patient Management System (CPMS) has already resulted in more harmonised and interoperable data being collected for specialist virtual reviews. But the area of registration holds possibly the greatest potential in terms of advancing research and understanding.
Registries are essential tools for generating knowledge about rare diseases, and -depending on the data they collect – can serve multiple purposes.11 Notwithstanding the variety in scope of the 24 ERNs, there have been robust attempts to ensure a baseline compatibility and interoperability via a concerted European approach. The best example of the latter is the European Platform on Rare Diseases Registration, initiated in 2013 by the European Commission’s Joint Research Centre in collaboration with DG SANTE. An important component of this platform is the ERDRI or European Rare Disease Registry Infrastructure.12 ERDRI seeks to make data held in rare disease registries searchable and findable. It does this via a suite of tools: the European Directory of Registries (ERDRI.dor); a Central Metadata Repository (ERDRI.mdr); a Pseudonymisation Tool (ERDRI.spider); and a Search broker (ERDRI.sebro).
The creation of a European platform to increase the reuse potential of precious rare disease data was an important step, given the variety of registries which exist (845 globally, according to Orphanet) but also the fact that only 1000 of the known rare conditions are included in at least one of those 845.13 Into this complicated ecosystem, the creation of ERN registries -or platforms to link new ERN registries with historical or possibly new disease-specific registries- holds major potential for advancing knowledge and better care, but also naturally for stimulating and advancing research. Supported by projects like the EJP RD14, ERICA15, and now ERDERA16, attempts are being made to ensure a certain level of interoperability in terms of the data collected in these new ERN registries. For instance, the Common Data Elements issued by the ERDRI were turned into a richer data dictionary under the EJP RD: this is just one example of efforts to make registry data FAIR (Findable, Accessible, Interoperable, and Reusable). Greater value will come with the advance of individual ERNs agreeing and standardising domain-specific datasets.17 5 of the ERNs received EC funding to develop their registries early on in the ERN story with the remaining 19 receiving their funds via the 2019 work programme of DG SANTE. Although still relatively young registries, the number of patients enrolled is increasing (and now exceeds over 95000). Different ERNs are approaching their registry set-up/linkage in different ways and increasingly, tools are being created to optimise their potential (see below).
Beyond the registry space, the fact that ERNs connect so many of the leading centres of expertise for rare disease across Europe also offers huge potential to increase the standardisation and reuse potential of electronic health data – rare diseases are a natural beneficiary of the anticipated EU Health Data Space.
ERNs are networks centred on patients
Patients sit at the heart of the ERN concept (and indeed, the concept emerged largely from the patient community in Europe). The Addendum to the EUCERD Recommendations stipulated that patients should have a meaningful role in all levels of ERN activity, governance included. To facilitate this, EURORDIS created the concept of an ePAG – a European Patient Advocacy Group18– to work with each ERN. Over 300 ePAG advocates have been approved and are working closely with the Network most connected to their particular condition. ERNs have conducted surveys on people living with rare conditions under their Thematic Grouping which is helping to understand patients’ needs and realities better than ever before. Just as clinician networks are growing under ERNs, so patient communities across Europe are coalescing around the ERNs, making it easier to engage patients and develop patient partnerships in research and care (though challenges persist).19 The ePAG advocates address cross-cutting issues together, across ERN boundaries, and their existence constitutes an excellent opportunity for external stakeholders to work with networks that are genuinely patient-centric.
ERNs offer Independent Expertise
Another advantage of the ERNs, for industry, is the fact that these networks -which as above, should be considered permanent, for all intents and purposes- are established independently of any industry influence. Companies often remark that the existence of structures and networks like this, assembled by the communities themselves, can be helpful in avoiding any accusations of bias.
Important Resources to Showcase the Power of ERNs for Research
Together4RD Webinar
One important resource, to showcase the value and advantages of ERNs as partners for research, is the webinar organised jointly by Together4RD and the European Rare Disease Research Coordination and Support Action consortium (ERICA) in late 2024
Resources Created by/With the dedicated ERN Research Action, ERICA
The ERICA website is actually an important gateway to ERN resources, especially pertaining to research. This 4-year project was specifically designed to advance ERN research, and has developed resources to improve various aspects of rare disease research (e.g. developing more effective data collection strategies, optimising patient involvement etc.). A few key resources generated by ERICA are linked below.
1st Monitoring Report on ERN Registry Data Collection
In terms of understanding the development choices, progress, and potential of the ERN registries, the 1st Monitoring Report on ERN Registry Data Collection (updated in 2024) is a useful resource
https://erica-rd.eu/wp-content/uploads/2024/11/ERICA_D2.5_02_24_NEW.pdf
Informed Consent Form templates
Informed Consent Form templates were created via the European Joint Programme for RD, EJP-RD, specifically for ERN registries. The templates can be adapted at ERN, national and site level, and include versions for patients and for parents/legally-designated representatives. They have been translated into 26 languages.
Data Sharing Agreements
Data Sharing Agreements. In a centralised registry, where all the data collected by a ERN centre is transferred to a centralised server, a Data Sharing Agreement should be signed between the registry and every HCP contributing data. A customisable Data Sharing Agreement template was developed for the ERNs, for this purpose.
The ERN registries have established Data Access Committees
The ERN registries have established Data Access Committees. If such a Committee agrees to grant access to the registry data to an external stakeholder, a data transfer agreement should be signed between the registry and the data requestor. A customisable Data Transfer Agreement template for the ERNs has been developed in the framework of ERICA, for this purpose.
https://erica-rd.eu/work-packages/data-collection-integration-and-sharing/generated-documents/
Patient Reported Outcome Measures are very important in rare diseases.
Patient Reported Outcome Measures are very important in rare diseases. ERICA has developed a PROMs Repository – as the first attempt to identify and centralize Clinical Assessment Outcomes questionnaires of relevance for rare diseases. This Resource has been created through the joint collaboration between Orphanet, Mapi Research Trust/ICON and ERN EuroBloodNet (VHIR, APHP), with the active contribution of ERNs more widely, and ePAGs. The repository should be regarded as ‘a centralized and standardized access gate to more in depth information contained in PROQOLIDTM.’
ERICA delivered a series of webinars of relevance to clinical trials in rare diseases
ERICA delivered a series of webinars of relevance to clinical trials in rare diseases. Some were developed within ERICA itself, whilst others showcase partnerships with other initiatives such as c4c. Some of these webinars should help external stakeholders to become more familiar with the ERNs.
The status quo of ERN registries
The registries established by the ERNs are perhaps particularly attractive resources for stakeholders who might be considering partnering with the ERNs for a range of research- related activities. The ERICA project generated a report, updated in late 2024, which summarised the status quo of these registries, in terms of the different approaches ERNs have taken to creating these infrastructures, the number of patients registered to-date, the size of their respective data dictionaries, and more. This report is linked in the ERICA resources table above, but is highlighted here too.
Amongst the highlights of this important report are the following:
- Most ERNs have opted to establish a core patient registry, using a centralised system (20 registries).
- Others have established/integrated multiple registries, or are in the process of doing so. Therefore, the number of ERN registries (29) actually exceeds the number of networks (24).
- These multiple registries are sometimes embedded within the same infrastructure of the core registry (e.g. as is the case of the subregistries in ERKNet, the ERN for rare renal conditions), or else have been implemented separately, often following different design principles (i.e., centralised vs. federated in VASCERN, the ERN for rare vascular diseases).
- Occasionally, multisystemic diseases are ‘shared’ under the scope of 2 or more ERNs; therefore, some ERNs have chosen to collaborate in shared patient registry projects. For example, the Core Registry, originally established as part of the European Registries for Rare Endocrine and Conditions (EuRRECa) project, now supports the activities of both EndoERN and ERN BOND. In these cases, collection of shared data elements is supplemented with the inclusion of more specific condition-dependent modules.
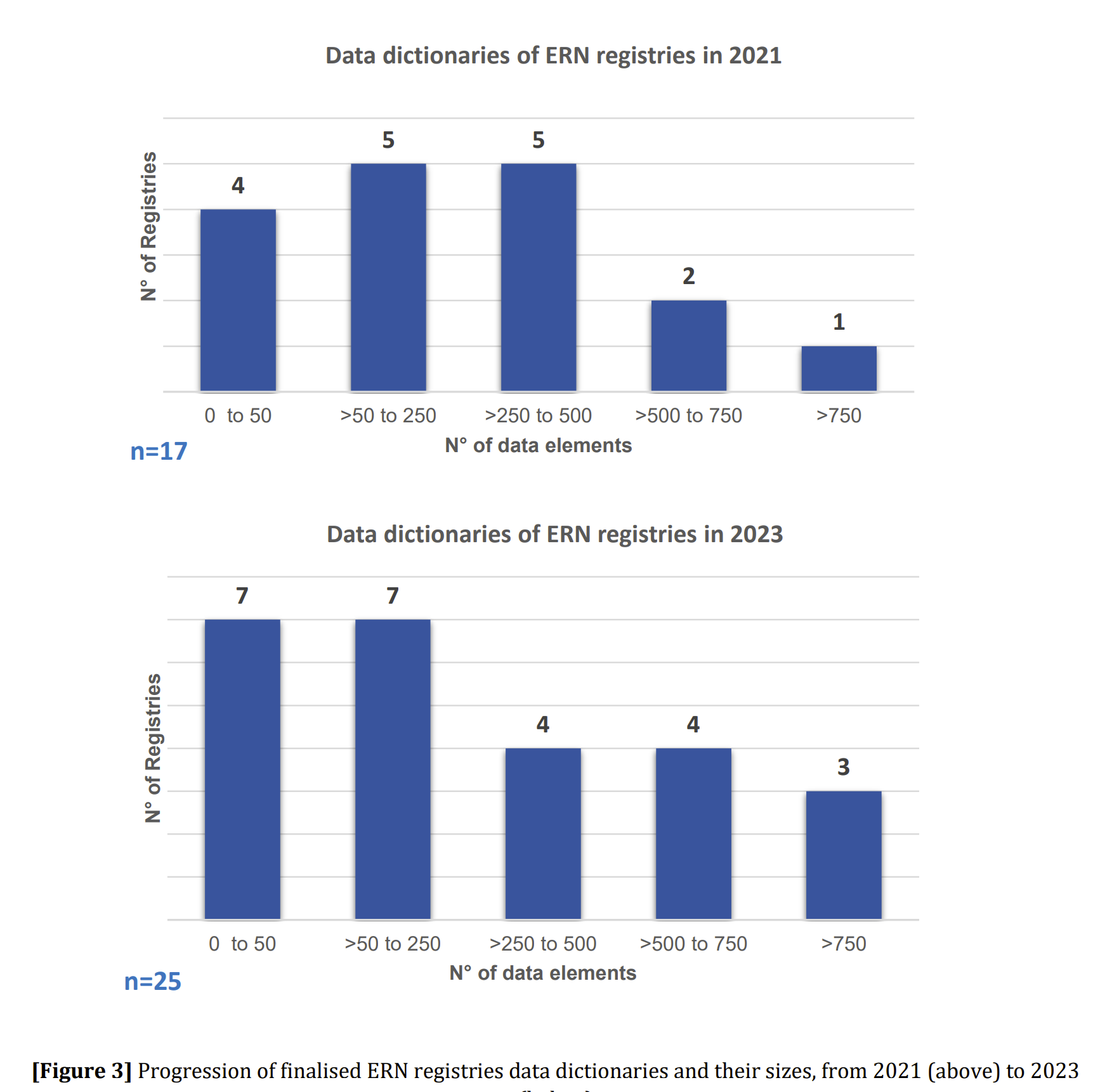
- Most ERN registries use external software solutions, including Molgenis (3), Castor (7), and RedCap (4), as well as other providers (10). Only a minority of ERNs have decided to develop their registries in-house (5).
- ERN registries have been steadily increasing their data dictionaries. Whereas in 2021, 8 registries had data dictionaries with over 250 data elements, in 2023 that figure was 11 (see figure on previous page).
- The type of data items collected by ERN registries is quite broad – whereas all collect clinical data, and almost all collect phenotypic and genotypic data this figure, few collect imaging, QoL or PROMS data at present.
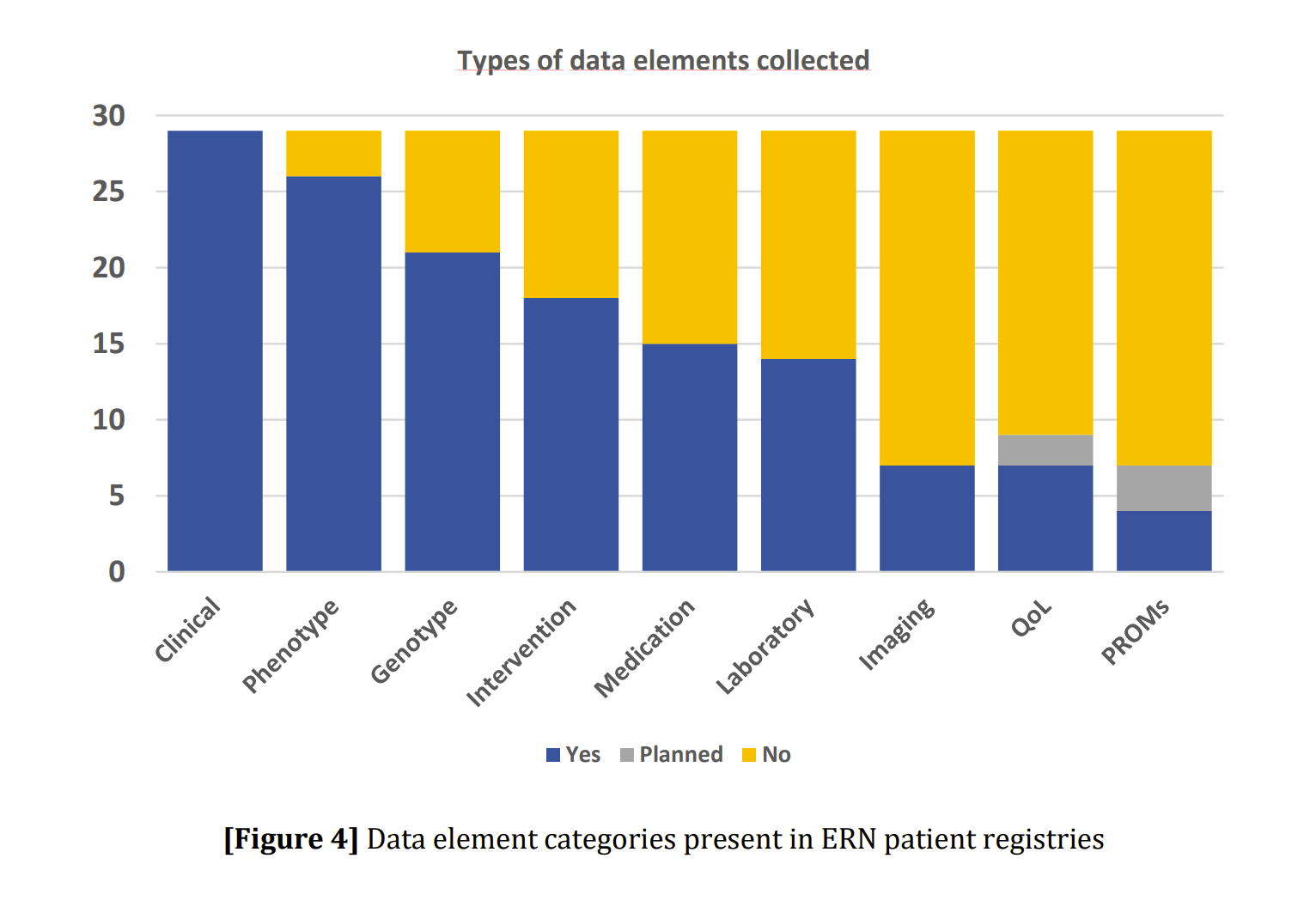
Related Resources
Together4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceThe resource explains that European Reference Networks (ERNs) are a major EU healthcare and research infrastructure that bring together clinical expertise, data and specialised resources across Europe to tackle rare and complex diseases and are valuable partners for collaborative research activities. It emphasises the untapped potential of ERNs to engage with the pharmaceutical and biotech sectors, advocating for greater awareness and public–private partnerships to accelerate rare disease research and development and benefit patients
View this resource Bookmark this resourceForging a successful collaboration entails all parties understanding and appreciating each other’s needs, priorities and realities. The needs and priorities of ERNs, on the one hand, and Industry, on the other, are quite different, in many respects.
It is important for ERNs to understand the motivations, requirements and priorities for private sector organisations, especially perhaps for stakeholders (whether researchers, clinicians, patients, or otherwise) from disease communities which have not worked extensively with Industry to- date, and for whom, therefore, public-private collaborations are very new.
Several helpful resources exist to build awareness of the needs and priorities of private sector organisations in the context of public private partnerships or collaborations; and although not always specific to ERNs, the messages therein are useful for ERN stakeholders.
One essential message to convey is that Industry brings more to a partnership or collaboration than simply financial resources. A dedicated webinar hosted by Together4RD and ERICA (the European Rare Disease Research Coordination and Support Action) in early 2025 highlighted what industry can bring to partnerships and projects beyond funding, and provided attendees with concrete examples of how industry has brought value to research projects conducted with ERNs in recent years:
A useful resource for understanding some of the needs and realities of the private sector, specific to working in rare diseases (if not specific to working ERNs), is a 2021 report prepared for EFPIA (the European Federation of Pharmaceutical Industry Association). This report, entitled ‘Addressing unmet needs in extremely rare and paediatric-onset diseases: how the biopharmaceutical innovation model can help identify current issues and find potential solutions’ focuses on medicines’ development, but is helpful in conveying the complexity and risk for companies working in this area.
- For instance, it explains how Industry is central to medicines’ development, and illustrates the high costs of drug development, the timescales involved, and the high failure rates – all of which made developing medicines a very risky enterprise, from an investment point of view, not least in areas such a rare disease which carry particular challenges of their own. “When making investment decisions, companies first consider the scientific opportunity, then examine commercial viability within the policy environment”. Key aspects of the decision-making process are explained.
- The report summarises some of the additional challenges of seeking to develop medicines in extremely rare diseases, knowing that 80% of all rare disease patients are affected by one of the approximately 150 diseases with the highest prevalence, but that 84.5% of the conditions classed as rare have a prevalence of lower than 1 in a million and affect only 0.33-0.55% of all people living with a rare disease. It explains why, as a rule of thumb, the rarer the disease, the more significant the scientific and commercial challenges inherent to rare disease therapeutic development.
The International Rare Disease Research Consortium, IRDiRC, has recently released a report which is extremely valuable in helping to convey the benefits which Industry can bring to a collaboration (and, in connection with this, illustrating the needs and priorities of the private sector).
This report ‘The different contributions of the industry in Public-Private Partnerships in Rare Diseases Research continuum’ stems from a collaboration between EFPIA, the Rare Disease Moonshot, and the IRDiRC Companies Constituent Committee. It highlights “the unique value pharmaceutical and biotech companies bring to Public-Private Partnerships”, providing four key takeaway messages:
- Scientific & Regulatory Expertise
Companies provide cutting-edge infrastructure, data, technical know-how, and a deep understanding of regulatory pathways. - Operational Capacity
With a global footprint and strong project management skills, industry partners help scale innovations, manage risks, and drive efficient implementation.
- Collaborative Leadership & Patient-Centric Approach
Industry actors know how to meaningfully engage patient organizations early in the R&D process, supporting co-creation of impactful solutions. - A Strategic Role in Rare Diseases
In a fragmented and resource-scarce field, industry involvement helps connect the dots, enrich efforts with real-world data, and accelerate impact.
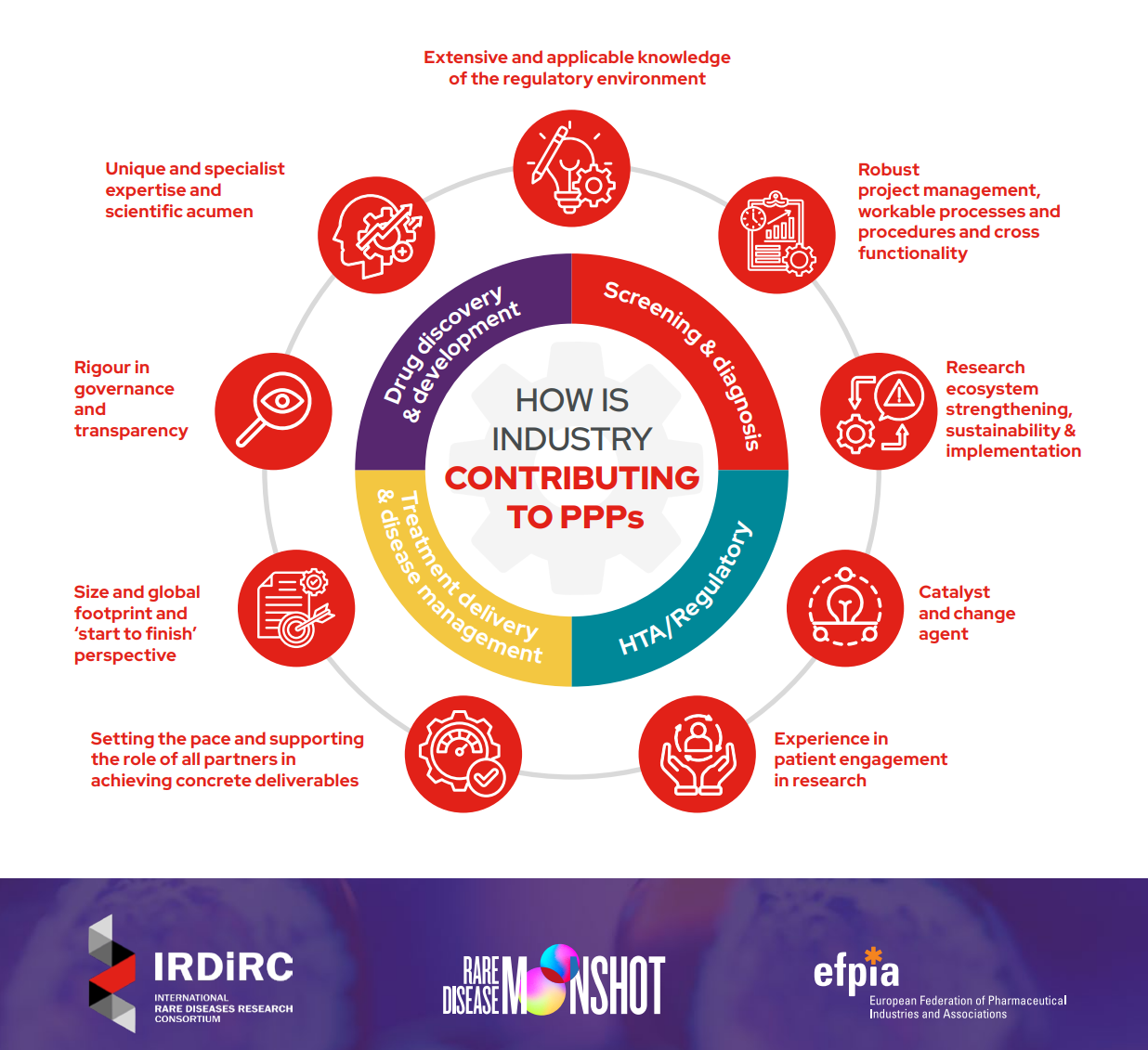
Last but not least, other tools within this Together4RD Toolkit serve to illustrate the needs and priorities of the private sector, when considering or embarking on public private collaborations or partnerships with ERNs; in particular, Tool 9 ‘Report on the Experiences and Learnings from the first ERN-Industry pilots supported by Together4RD’ and Tool 10 ‘Key recommendations for both ERNs and Industry from the experiences of the first ERN-Industry pilots’. The latter includes recommendations to support an effective partnership, and there are several layers to this; however, some
of the points in this document relate specifically to the need for non-Industry partners to understand certain parameters and realities for private sector partners, such as the following:
- Understand that public and private actors tend to place value on different sorts of outputs.
- Consider how research can result in wider impact, beyond publications, in terms of changing patient pathways and diagnostics practice, and outcomes beyond publications.
- Acknowledge that companies in the rare disease space may have goals and vision to improve the wider rare disease ecosystem, beyond simply developing and selling a product.
- Accept that industry partner(s) will wish to have input to the scientific development of a project plan and should be viewed as an equal partner. Indeed, this should be welcomed, as it will bring significant advantages to the research, as it will bring access to the vast in-house scientific expertise but also expertise in medicines development, HTA, data science, and much more.
- Have realistic expectations of both the level of resources industry can contribute to projects, and the way in which it does this. Avoid thinking of companies as purely funders of research. Companies are generally unable to dedicate large sums of money, for the subsequent definition of a detailed project plan – in fact it is the reverse: funding can only be found, internally, based on the contents of a proposed plan. Companies do not award funds as unrestricted grants, without any direct involvement.
Related Resources
This webinar highlighted how industry contributes to PPPs beyond funding, and provided attendees with examples of how industry has brought value to research projects conducted with European Research Networks (ERNs) in recent years.
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resource
This pilot project centres of three main activities: Firstly, value will be drawn from several sources of existing data relating to patients with the rare bone condition OI, to better elucidate the natural history and the disease burden. Genotype- phenotype correlations will be explored, as part of this drive to better understand the condition.
Secondly, prospectively, the project will measure the impact of disease on patient activity and quality of life using digital technologies in a real-world setting, through a combined approach of gait analysis and sensors.
Lastly, in preparation for smoother regulatory pathways for OI therapies in future, the project partners will jointly engage in early scientific dialogues with other stakeholders (such as regulators and HTA), to gain insights into approaches to foster patient access to innovative medicines.
Who is involved? EuroBloodNet, Innova, ENROL and Takeda in partnership

This initiative is all about improving the diagnostic pathways for rare haematological diseases by utilizing AI algorithms for early detection. The activity is expected to focus on thrombotic thrombocytopenic purpura (TTP), a very rare and debilitating condition existing in both a congenital form and an acquired, immune-mediated form (which manifests in the 4th or 5th decades). The variable phenotype for TTP and lack of availability of the necessary diagnostic tests, leads to delayed diagnosis, which is very concerning as without a correct diagnosis and treatment, organ ischemia and death occurs in around 90% of cases.
To improve early diagnosis, the plan is to employ an AI federated platform across key clinical centres, which will ideally be based on the hospitals own EHR systems. Whilst reducing time to diagnosis, and thus enabling treatment to begin as early as possible, the AI platform should lead directly to improved patient outcomes by alerting treating clinicians of patients at risk of relapse, who can then be monitored in appropriate ways.
The initial phase of the pilot will focus on scoping activities and identifying centres for the implementation phase. From the ERN side, the pilot is being delivered through an organisation known as the EuroBlooNet Association, together with the Fundació Hospital Universitari Vall D’Hebron, which is the entity in charge of the ERN’s shared registry (ENROL), and also the Fondazione IRCCS Ca’ Granda – Ospedale Maggiore Policlinico.
Who is involved? Novo Nordisk, ERKnet and OxalEurope

The RHINE Project aims to improve care pathways and patient outcomes in rare renal conditions, by building on existing registry infrastructure, especially the core registry of the ERK-Net ERN (named ERK-Reg). This pilot focuses in particular on an ultra-rare disease called primary hyperoxaluria (PH), and addresses a fundamental need to complement the core registry structure of the ERN with detailed data collection for specific conditions.
A ‘harmonization and interoperability’ model will be developed for PH, by establishing a Rare Kidney Network data registry, in collaboration with the European Hyperoxaluria Consortium (OxalEurope), to achieve seamless data connection across ERK-Net and PH-specific registries.
Through this new data linkage approach, the project aims to understand PH diagnostic and referral pathways locally, measuring metrics like time-to-diagnosis, where PH patients are seen (by measuring the number of cases in each referring center), and the percentage of patients diagnosed before they reach end-stage renal disease (the point at which the kidneys can no longer support the body’s needs). To compliment this focus on an improved data ecosystem, educational activities will be implemented at regional and local levels, to target the gaps and shortcomings identified. As of late 2024, this pilot has already generated significant added- value simply by bringing the registry owners from the ERK-REG and the OxalEurope consortia together, around the same table, having built a robust formal agreement for collaboration. The technical integration work is now underway, mapping data dictionaries to explore what each registry ecosystem currently collects.
As part of the significant preparatory work leading up to the submission for publication of the Together4RD Position Statement, Together4RD sought examples of ongoing or past public private partnerships in the rare and highly specialised healthcare field. The reason for this information gathering was three-fold:
- To ameliorate any concerns within the ERN Board of Member States (BoMS) about public private partnerships in this field
- To collect learnings on the set-up and delivery of the activities involved.
- To inspire ERNs and Industry (especially in less research-mature fields) as to the kind of activity ERNs might enter into with Companies
These case studies tended to fall into two categories – registry-connected, or else concerned with advancing clinical research broadly, outside of clinical trials specifically. They were presented in brief as part of the supplementary material for the Together For Rare Diseases Position Statement.
Related Resources
This Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceThis case study highlights the achievements of a specific community, namely the neuromuscular field, in establishing both registry-related and broader clinical research activities involving partnerships with Industry.
TREAT-NMD was established back in 2007 as a European ‘Network of Excellence’, via an FP6 grant, in order to advance trial-readiness in all neuromuscular diseases. It has played a key role in bringing together the right experts – patients, advocacy organisations, healthcare professionals, researchers, AND pharmaceutical organisations – to drive progress. It has created a suite of tools and activities to achieve its goals, and in 2019 was ‘spun out’ of Newcastle University (the original grant holder and thus Network coordinator), as its own legal entity. Many key resources were established under that initial grant, to help extend translational research, these include:
- cell and animal standard operating protocols (for preclinical research);
- a unique advice service, TACT
(the TREAT-NMD Advisory Committee for Therapeutics) - global patient registries
- care guidelines, and family guides
- and more
From the early stages of TREAT-NMD, Industry has always been acknowledged as a key stakeholder and driver of treatment development. In the original project phase, companies were included as members of the consortium, to ensure the tools developed during the grant funded period actually met the needs of industry. Consequently, many of the activities and outputs listed above involved close public-private collaboration, and ethically-robust practices and codes have been developed to facilitate this.
One key area of TREAT-NMD Industry engagement concerns patient registries, to improve understanding of disease, help build trial-ready patient cohorts, and boost patient recruitment. TREAT- NMD created tools and approaches to connect numerous autonomous registries for the more common neuromuscular diseases (NMDs) NMDs like DMD and SMA. To create greater interoperability and increase the power of standalone registries for these conditions, TREAT-NMD developed both core and expanded datasets to standardise data. At the same time, TREAT-NMD coordinated the creation of global patient registries for rarer NMDs, for which one single registry worldwide makes better sense. The result of all this work is a network of inter-connected registries able to provide a wealth of information, which can be queried by academic sites (for free) or by Companies (for a fee). Industry have purchased anonymised data of this sort for many years, which supports feasibility studies or enables patient recruitment in clinical trials. The model established back in the days when TREAT- NMD was coordinated by Newcastle University saw those funds from Companies invested back into the core staff involved in running the network, and/or to support networking of the registries themselves. Now that neuromuscular therapies are approved, TREAT-NMD Services Ltd (a dedicated legal entity which spun out of Newcastle University in 2019) is expanding the registries to be able to carry out Post Marketing Surveillance on a global scale.
These days, there are 65 registries collaborating with TREAT-NMD as the ‘TREAT-NMD Global Registry Network (either for NMD generally or for a specific condition) and they together collect data on approximately 88,800 people living with an NMD. Many of the processes initially established under the days of the TREAT-NMD network remain in place, to support Industry interactions. One major form of interaction with Industry concerns access to registry data. When a Company wishes to purchase data from the global registries, for instance to perform a feasibility assessment, the requests are considered by a committee set-up very early on in the TREAT-NMD lifetime – the is the TGDOC or TREAT-NMD Global Registries and Data Oversight Committee. It has been very important to TREAT-NMD, both as an initial Network of Excellence funded by the EU, and now as a ltd company, as well as its ‘in-between’ stages, to ensure Industry interaction around accessing registry data is appropriate and handled robustly, recognising the key importance of this stakeholder group but also acknowledging the need for the highest ethical approaches. Tools have been developed to support this, and build transparency, such as the TGDOC Charter. However, the engagement has been far more substantial than individual Companies simply purchasing data (whether as a one-off or on a longitudinal basis). Crucially, TREAT- NMD has always partnered, and continues to partner, with Industry on all activities, as appropriate, to ensure the end products and outputs will be useful to Industry – and this is very much the case with the registry-related activity. For instance, Industry experts are always consulted when core and expanded datasets are being developed or updated for the individual conditions, to ensure the needs of Companies are reflected in the type of data being collected, and that the way in which the data is being collected is standardised and appropriate.
Beyond the registry-related activities, TREAT-NMD engaged with Industry to advance clinical research via other means. One important tool developed by the initial Network of Excellence is the CTSR (care and trial site registry), which was designed to provide information on personnel facilities, patient populations, and prior experience with conducting clinical trials. Sponsors can use the resource to help select experienced trial sites, and provided input to its original creation.
Another key resource -which is perhaps more in the category of ‘Industry as a customer’ rather than a co-creator- is the TREAT-NMD Advisory Committee for Therapeutics (TACT), which allows a better prioritisation of compounds to be taken from preclinical studies into clinical trials. TACT was established in 2009 to de-risk trials and ensure compounds moving into clinical trials have the best possible chance of making it to patients. Anyone can apply for a TACT review, and the goal is to help the applicant – commercial or otherwise- to position a candidate therapy along a realistic and well-informed pathway to clinical trial and eventual registration, by identifying potential pitfalls in the translational process and by providing transparent advice. Each application is given a bespoke international expert panel made up of preclinical, clinical, regulatory, patients and industry experts. Where the application is a Company, there is a fee for this advice and the report which follows an in- depth real-time review meeting. The way the model was set-up under the TREAT-NMD network saw all funds raised in this way being used to support the core running of TACT. Naturally, a high level of confidentiality is maintained.
Other TREAT-NMD interactions have included Industry funding training events, summer- schools and educational webinars (without playing a direct role in setting agendas).
In terms of the mechanisms of governance for Industry interactions – in the original grant, everything was covered by confidentiality agreements within the project consortium. Outside of this, and in the years since that grant came to a close, bespoke contracts and agreements have been set in place, such as the TGDOC Charter to govern the registry enquiries, as above, CDAs (Confidential Disclosure Agreements) and other contracts. The way in which contracting has worked has changed over the years. These days, TREAT-NMD is a not-for-profit organisation and its own legal entity, and so can undertake contracting directly with any given Company. For many years, however, when the TREAT- NMD Network was NOT a legal entity, contracting was performed by and centred around Newcastle University, as the representative of all the other entities involved in the network. This was not ideal, in some ways, as it meant the University legal department had to be brought on board and learn how to do this kind of work, which is not always obvious (especially in risk- averse organisations). Some of the processes involved in contracting and handling funding, for instance, were more bureaucratic than the experts involved would have liked. This was one of the reasons, in the end, that TREAT-NMD became a spin-out. However, the key point is that a great deal of collaboration was possible through this model of a non-legal-entity network, with one party (which was a legal entity) acting on behalf of the rest.
In summary, TREAT-NMD has been very influential in advancing clinical research in the NMD field. Considering the activities and collaborations with Industry summarised above, an important ingredient for success was building a truly multistakeholder network and community from the start, which entailed recognising the value of Industry as a stakeholder, even in the early days. The approach was very much to develop any and all tools which would have a relevance to Industry, WITH Industry, and also ensuring an international and global approach.
This is an example of a national registry for a particular condition, established by Industry as part of a multistakeholder collaboration.
The main treatment for Pompe Disease is enzyme replacement therapy (ERT), and Sanofi provides two ERT products – Myozyme, approved almost 20 years ago, and Nexviazyme. This national registry was first qualified by the French National Committee for Rare Diseases Registries (CNR-MR) supported by INSERM and institut national de veille sanitaire (InVS), in 2008, to collect prospective clinical, functional and biological data on all French patients with a Pompe disease diagnosis (whether treated or not). The different stakeholders first discussed need and goals for the registry, and, after agreeing a plan, Sanofi established contracts with a group of French hospitals (individual contracts with each), to obtain consent from patients and provide the data. These contracts are updated on a one-to-one basis, as needed. Funding is provided by Sanofi to the research teams of the hospital, to support the data entry, but is also supplemented with funding from the French Association against Myopathy (AFM), French Glycogenosis Association (AFG), INSERM, and InVS. The registry serves multiple purposes:
- Elucidates the natural history of Pompe disease
- Enables the medical community to develop patient monitoring recommendations
- Optimises patient care
- Enables an assessment of the long-term effectiveness of the ERT
The results of the Registry data collection are published annually. Details of the registry dataset and patients enrolled are available here.
Key to success here was the fact that both main parties (the hospitals and Sanofi Genzyme) were ‘on the same page’ and saw value in the proposal. In terms of challenges, the need to contract with each hospital can be time-consuming. Furthermore, when regulators request data from the Company, regarding the ERT, it is the individual clinicians who are actually having to provide the data – in other words, the data access process could be improved.
This case study is an example of how one of the registries created by the ERNs, for rare renal conditions, has interacted with Industry in its early years.
ERK-REG is the registry of the ERKNet ERN, for rare renal diseases. It was initiated in 2019 and acts as a single core registry for all rare renal diseases. The Registry collects data from the HCPs which are part of the ERN and is able to serve multiple purposes:
- Epidemiology of rare kidney diseases Information on level of diagnostic ascertainment (inc. access to genetic testing)
- Phenotype and natural history information
- Continuous monitoring of diagnostic and therapeutic performance and guideline adherence for optimized patient outcomes
- Rapid identification of patient cohorts for clinical trials
Early collaborations with Industry (i.e. prior to the Together4RD pilots) included ERK-REG brokering contracts between an Industry sponsor and sites that have patients eligible for clinical trials. Another example involved contracting with large pharma to provide aggregate data on over 200 paediatric patients receiving a medicine off-label (which was used as supportive evidence for a Paediatric Investigation Plan). There is an aspiration to use fully anonymized patient-level registry data to create external control arms for clinical trial, in future.
By 31st December 2023 a total of 22,687 patient records had been included in the ERK-REG (8928 by adult units (39,4 %), 13,758 by pediatric units (60,6 %), across 53 ERKNet Member centres, 5 Affiliated Partner centres, and 42 other external centres – see here.
This case study involves Industry accessing a key registry established by a non-profit society, and using that data for a range of regulatory purposes.
The EBMT (European Society for Bone and Marrow Transplantation) is a non-profit Society founded in 1974. Originally, the scope was purely clinical bone marrow transplantation, but more recently, cellular therapies have also been included. It is a collaborative network for professionals working in centres and individuals in field of HSCT, gene and cell therapy – it has over 5000 members in over 70 countries, including over 600 transplant centres (covering >90% of all transplant centres in Europe).
The three pillars of the EBMT are research, education, and patient care. The EBMT Registry is the backbone of EBMT’s research and educational activities. It contains patient clinical data, including aspects of the diagnosis and disease, first-line treatments, haematopoietic stem cell transplant (HSCT) or cell-therapy-associated procedures, transplant type, donor type, stem cell source, complications, and outcomes.
EBMT provides data to its members (ranging from individual physicians and nurses to Centres) and is able to perform studies and assess epidemiological trends. Industry are long-time collaborators in the EMBT broadly. Companies can become partners of excellence, without voting rights. If they wish to participate in one of the EBMT scientific studies, using the Registry, they negotiate payment. Of particular note is the success in gaining EMA qualification (specifically of the cell therapy module): to- date, EBMT has made various agreements with Companies on a one-to-one basis to support their Post Authorisation Safety Studies, based on secondary use of the Registry data. At present, no direct access is provided to the Registry data – rather, Companies approved as partners of excellence can access data collected in reports. In addition, Companies can contract for individual research projects, such as feasibility reports, surveys, conducting retrospective or prospective studies, etc. Where possible, only anonymous data is shared (although pseudonymised data can be shared with explicit patient consent). The Registry facilitates over 100 publications per year.
This is an example of a national (French) initiative to promote more rare disease research collaborations between the public and private fields
The POC Club is a national (French) resource to promote innovative research and develop new treatments for rare diseases by offering coaching and guidance for researchers and clinicians and, crucially, connecting them with suitable Industry partners. Established in 2017, it is recognised in the 3 rd French National Plan for Rare Disease. POC is essentially an effective business model, based on a research valorisation tool & implemented through a group of industry partners. The initiator for the idea was the Foundation Maladies Rares, and the goal was to bridge the gap between academia and industry in rare disease. POC Club is financed through company partners and wider fundraising. Webinars allow academics to present 10 minute ‘elevator-pitches’ for projects they wish to conduct, and the Industry feasibility of the research proposals is assessed. They run two sessions per year – over the first 5 years, 85 projects have been presented to Industry through the POC Club, with 70 connections made, and an 80% interest rate from the Industry participants. If a project is taken forward by a Company, partnership agreements can be signed between the key actors and a tech transfer office.
The first success of the POC was the creation of a partnership (signed in April 2018) between industry, an academic researcher, and a Tech-Transfer Office, to develop a gene therapy for Fragile X Syndrome.
This partnership led to an Exclusive Worldwide License Agreement in 2021. Factors for success in this arrangement included:
- The stakeholders coming together at an early stage in the research
- Each partner contributing with their unique experience and capabilities, and valuing what the other could bring
- An understanding of the expectations and constraints of the other partner
- A neutral and trusted third party to initiate and facilitate the partnership
The POC Club has encountered several challenges in attempting to establish collaborative projects between academic researchers and Industry. For instance, there are different expectations from Industry depending on the size of the company – large pharma companies have different needs, perspectives and expectations to small biotech companies. The gap between academia and industry is very much real, and has to be addressed. In particular, academic researchers are not aware of the expectations and constraints Industry has to deal with. It has proven very important, therefore, to coach researchers and clinicians to better understand the key milestones of drug development. POC Club plays an important role by acting as a third party to facilitate the discussions and help move things forward (especially when addressing IP matters).
This is a well-established case study from the paediatric cancer community, dating back over 20 years, in which Industry is a long- term collaborator in efforts to improve the whole lifecycle of product development in paediatric oncology.
The Consortium involves 63 Paediatric Oncology Departments in 18 European countries with expertise in conducting early phase trials in children and adolescents, together with 25 European research laboratories. ITTC launched in 2003, long before the Paediatric Cancer ERN (ERN PaedCan). ITTC is a non-profit organisation established under French Law. The goal is to accelerate the introduction of new, effective, and safe therapies for the treatment of children and adolescents with cancer. The ITTC offers a wide range of collaborations with Industry, across the whole lifecycle of product development, from early portfolio evaluation to advice on generating phase 1 data, through to support with paediatric trial design and finally implementation. In this way, ITTC increases the likelihood of the most effective therapies entering development, optimising the chances of these medicines eventually becoming available to patients.
This case study concerns a relatively new collaboration across Europe, to improve clinical trials in epilepsies, with strong ERN engagement and leadership
ECET was launched in 2021 by the regional Executive Committee of the International League Against Epilepsy (ILAE-Europe), and was endorsed by the ERN EpiCARE, the European Consortium for Epilepsy Trials. The goal is to provide advice and expertise to optimise the design and implementation of clinical trials in epilepsies across Europe, for both adults and children. Despite the approval of numerous antiseizure medications, many individuals with epilepsy syndromes continue to experience seizures, suffer from comorbidities, or experience adverse events. Well-designed trials are essential to provide the necessary evidence for rational treatment choices in rare epilepsies, but historically, antiseizure treatment trials have been poorly designed. There remains a critical need for well-powered and representative clinical trials to develop novel treatments that can enhance quality of life, reduce seizure burden, minimize adverse effects, lower healthcare costs, reduce the risk of sudden unexpected death, and ultimately, modify the natural evolution of the underlying aetiologies.
ECET is a collaborative group of European investigators with shared interests and a good track record in designing and performing epilepsy trials. These experts have links to over 80 centres across 35 European countries. The priorities include innovative trial design and outcome measures; genetics and targeted therapies; epileptogenesis and disease modification; epilepsy surgery outcomes and follow- up; and more.
ECET offers a range of expert services to both academia and Industry, including the following:
- Leading and supporting natural history studies
- Promoting precision medicine
- Advice on clinical drug development
- Advice on trial design
- Selection of trial sites in Europe
- Centralised/standardised adjudication processes to reduce variability in multicentre trials
- Organising educational activities to enhance the skills of researchers and healthcare professionals.
The ECET is still in its early days, but structures are being develop to contract with pharma companies and CROs. Importantly, the ECET is now an established legal entity.
Another long-established case study from the paediatric cancer community, which centres on multistakeholder meetings
The ACCELERATE Consortium was initiated in 2012, in the paediatric cancer field. The goal is to accelerate the process of developing and evaluating innovative therapies for children and young people with cancer. Pharma companies participate in the activities, which are essentially multistakeholder fora in which the group analyses the state quo of research and development and identifies activities necessary to drive forwards the pace of progress. Industry representatives are part of the Steering Committee, as equal partners, and Industry is part of projects designed to push the field forward (which include education and working groups on clinical research topics, but not specific trials).
One barrier to ERN-Industry collaboration, especially for research communities which have not traditionally seen significant R&D effort, and for Companies which are not very familiar with ERNs and what they have to offer, is a difficulty in envisaging tangible collaborative activities. The following tables of activities were originally created following lengthy Together4RD consultations with dedicated working groups, around existing public-private collaborative projects or activities in the rare disease space. The experts in these working groups were encouraged to identify and then analyse a range of such activities and brainstorm on their suitability for possible ERN and Industry collaboration.
Where relevant, examples of case studies advancing each activity, were included. For further details of these case studies, see Tool 7 ‘Case Studies – example of previous or ongoing public-private collaborations in the rare disease space’. These tables were originally included as supporting material for the 2023 Together4RD Position Statement, and have been further adapted in 2024-5 for this Toolkit. The contents are intended to be illustrative, though not exhaustive. Activities are divided into two broad tables – one relating to registries, which are key resources for the ERNs: the other is concerned with activities to support clinical research and knowledge-generation more broadly.
NB: Concerning clinical trials, please see the note below the tables. Together4RD has not prioritised a goal of fostering ERN-Industry collaboration in clinical trials, specifically. The Steering Group recommended a focus on less traditional activities one could envisage between Industry and ERNs, which could reasonably be expected to conclude within a year or two of initiation, in order to yield some early lessons to support more -and more effective- collaborations in future. Furthermore, there was a hope that targeting activities more in
the realm of building resources in a given group of diseases, or addressing barriers to R&D, might hold a greater potential for multicompany engagement and could generate added- value downstream for specific companies whilst also serving an important goal of enriching the wider rare disease research ecosystem. For instance, projects concerned with linking previously distinct data sources -e.g. by building interoperable registry platforms- could foster new research and drive new knowledge for the same or broader disease communities going forwards, whilst also answering the research question at hand. This kind of approach, in which stakeholders increasingly collaborate to put in place tools and advance knowledge able to drive progress and advancements across the wider rare disease research arena, is part of the ‘paradigm shift’ called for in the Rare2030 recommendations, and is very much in-line with more recent calls to embrace innovation in European therapy development.
Using registry data to understand the natural history of a disease or identify unmet medical need
“Longitudinal data collection can help to elucidate the natural history (NH) of a condition. Not enough is known about the NH of many rare diseases, which lack adequate registries to collect data (and often, for the rarest conditions, such registries need to operate at the global level). As registries are all about structured data, careful thought must be given to the initial data dictionary (including any associated mandatory recommended datasets), as it needs to be sufficiently broad to detect unknown effects as well as monitor known symptoms (i.e. without a robust starting knowledge of the NH, especially of complex, multisystem conditions, it may be that a meaningful dataset which should be monitored will not be recorded). Patient engagement in establishing registries to collect NH is therefore especially meaningful.
Related to this, registries hold the potential to illuminate unmet medical need; for instance, a registry dedicated to a rare lung or disease may capture other presentations or comorbidities that have not emerged in clinical trials, and which – in addition to elucidating natural history – therefore highlight unrecognised medical needs. It is important for companies to know the full clinical picture. However, it is also worth considering whether registries are the most appropriate sources of such knowledge – electronic health records (EHRs) possibly hold more potential here, or will, in future. The potential for ERN registries (as in, the new structures created by European Commission grants over the past 4–7 years) to elucidate NH will be variable, as many have opted not to collect large numbers of data items in the first instance, but are instead collecting data of relevance to all conditions under the scope of that ERN. Having said this, the data dictionaries of ERN registries are growing (as of late 2024, all but 6 ERN registries included over 50 items in their data dictionaries, with 7 including over 500 items). Plus, in addition to ERN registries, several manage disease-specific registries.”
Case Study
An example of a public-private collaboration here is the Sanoffi French Pompe registry, which has been prospectively gathering clinical, functional and biological data of all French patients with a diagnosis of Pompe disease confirmed by enzymatic and/or molecular analysis, whether treated or not – untreated patients can help to reveal NH of the diseases.
Using registry data as real-world data to serve regulatory purposes
“This is an often-cited goal for rare disease registries, but examples are quite challenging to find. One goal would be reducing the use of placebos in future trials by using registry data as a control arm. Such an activity is arguably more feasible and effective when data in registries is more standardised (and it is probably necessary to think less about ontologies, as has been the case with rare disease diagnostic platforms and project traditionally, and think increasingly of standards for data structure, such as OMOP Common Data Model, and perhaps standards specifically relevant for clinical trial data, especially CDISC). There is a real need for regulatory buy-in for these sorts of uses, and there is still perhaps quite a poor understanding of what sort of data is acceptable to the regulatory bodies for particular types of activity.
(The EMA has issued some guidance here.)
A recent workshop organised in Feb 2025 by the ERICA and conect4children initiatives explored the aspirations of ERN registries around supporting a range of regulatory purposes. There is a high level of interest in this kind of functionality, although almost all view this as being a future activity, something they envisage embarking on in 5 years’ time.
A key point here is, to serve this kind of ambitious use, registries need to be collecting the right sort of data – data which will be of use to Sponsors and Regulators. Some more specific forms of registry data serving as Real World Evidence are highlighted below.”
Case Study
ERK-Reg is a rare example of an ERN registry which has already begun to explore how its data could support regulatory activities. It has been able to provide aggregate data on over 200 paediatric patients receiving a medicine on an off-label basis, to be used as supportive evidence for a Paediatric Investigation Plan. This data broadens the evidence base especially for safety, but also the efficacy of the drug, to inform the regulatory process. The EBMT registry has received a positive EMA qualification opinion, making its cellular therapy module a suitable data source for regulatory purposes. Both therefore offer insights to this kind of activity.
Using registry data to conduct post-marketing surveillance (see also a related activity below)
This is another type of activity which tends to be viewed as highly desirable, but apparently happens little in practice at present. A key consideration here is that patient-level data would be required for this. It has long been a goal of registries to replace the need for Industry to create drug-specific registries, but Companies frequently reply that existing registries are not capable of meeting strict regulatory criteria. Therefore, a real partnership between the registry creators/managers, Companies, and the EMA, would be required. In particular, tools would be required to ensure the quality of data in registries. The EMBT registry case study should be illuminating here.
Case Study
EBMT has entered into various agreements with industry partners to support their EMA-mandated Post Authorisation Safety Studies (though even here, the studies are based on secondary use of EBMT registry data). The EBMT registry does include data quality checks that should promote consistency at the point of data entry, but there is no onsite Source Data Verification (SDV) or comprehensive remote SDV in terms of the entire registry as a whole; however, within the context of individual studies, additional quality checks can be performed (remote and/or onsite). The experiences of the few rare disease registries (EBMT and Cystic Fibrosis) which have received EMA qualification should be leveraged here, along with any guidance from the EMA Registry Taskforce. The TREAT-NM Registries Platform is also an interesting example, as here, the goal is, the goal is to enable multiple companies to fund a common platform for PMS.
Collaborating on defining data sets or data dictionaries
It is important to consider the purpose of a registry – what must it be able to do? The data one needs to collect for a simple epidemiological study will be less than (and different to) data required for Post-Marketing-Surveillance. Several projects are looking strategically and technically at how to increase the interoperability and FAIRness of registries (along with other sources of rare disease patient data), to try to allow data to speak with other data from other relevant registries, to serve particular goals. These activities (e.g. the work on making the ERN registries more FAIR under the EJP RD, continuing under ERDERA; the data tasks of conect4children which have explored how registry data could support better clinical trials or function as RWE in the paediatric space; and disease-specific projects like Duchenne Data Project in the Netherlands) present a number of important best practices. However, there has been less emphasis to-date on co-developing key resources like data dictionaries with Companies (partially because the ERNs have not felt able to do this to-date). Such activity, in the future, should include defining and implementing Patient Centred Outcome Measures within registries (aligning with work on PCOMs and PROMs under ERICA and the ERDERA, for instance)
Case Study
The TREAT-NMD registry work is one example of where companies have been involved in developing disease-relevant datasets and dictionaries for the global registries.
Use of registries to improve care
It is very much in the interests of companies to see the standard of care raised, which can happen when clinicians, researchers and patients use registry data to identify good practices and enshrine ‘what works’ into clinical practice guidelines or similar. Implementation of such guidance can create a more harmonised clinical ecosystem, which presumably then means a more equal baseline for patients with the same disease in different countries.
Case Study
A good example here comes from the DMD field: registry data enabled a good understanding of NH but also showed what worked, in terms of interventions – researchers could see that in countries where steroids were used, boys were ambulant for longer than in countries where they weren’t provided routinely, and night-time ventilation improved health and wellbeing significantly, etc. Those observations then made their way into international diagnosis and management guidelines, which are an important tool for standardising the level of care.
Use of registries to identify the best clinically-performing sites
Companies value knowledge about HCP/site expertise and outcomes. By benchmarking centres, companies can gain information of respective HCP outcomes, life expectancy etc. Registries can thus yield valuable information on regional and national performance and assist with decisions on which sites to contract with for clinical trials, as well as potentially supporting decisions on where to concentrate ATMPs provision. When it comes to identifying key sites for paediatric clinical trials, the mapping and resources created by the conect4children IMI2 initiative, which has now spun-out into a legal entity, the c4c Stichting, are also very important.
Case Study
The ERK-REG registry provides the ability to benchmark in this way, and other ERN registries are working towards this goal.
Using registry data to do feasibility assessments and trial planning
This is linked to the previous activity, but goes a step further.
Case Study
A good practice noted in the ERK-REG case study is the brokering of Sponsor contacts with sites that have patients eligible for particular clinical trials: the registry allows Companies to assess the feasibility of their studies. Another good example comes from the TREAT-NMD registries, which use a global network of autonomous registries (most using core and extended datasets to promote more harmonised and interoperable data). A system of checks and balances is in place to ensure companies can make a request to an oversight committee made up of curators of national registries for conditions like SMA and DMD. If this TGDOC, as it is called, approves the request, the data is collected from the registries (in aggregate form) and Companies can see how many patients they would likely be able to recruit in particular countries, how many patients meet particular inclusion criteria etc. This is very valuable in terms of letting Industry plan whether a trial is feasible or not and gives insight on how to structure it. The Companies pay for this aggregate data and the funds go back into the TREAT-NMD system, supporting the curators of the registries to meet and network, for instance. The EBMT also provides data for Companies, based on individual requests. Such research projects include (feasibility) reports, surveys, support for statistical analyses, performing retrospective or prospective studies (depending on the informed consent – specific projects sometimes require new informed consent forms, different to that requested when originally inputting data.) It is interesting to consider how registries might complement other approaches to identifying sites for clinical trials, such as the structures created for the paediatric community via conect4children
http://dx.doi.org/10.1016/B978-0-323-88459-4.00019-5
Industry funding registries or registry platforms
This activity may involve some or all of the activities specified above, but goes a step beyond, in one key way – here, Industry contributes resources to the setting-up, maintenance or expansion of a registry/registry platform. There are multiple benefits here, including the ability to avoid the creation of drug-specific registries. It would probably be necessary to think of a collaborative funding approach here, with modules for specific conditions. As yet, no examples were forthcoming from the Together4RD stakeholders, across the consultative activities, so this would very much be an aspirational future goal for the ERN ecosystem to explore.
Related Resources
In addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceThis Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceEnabling broad (all-ERN) multistakeholder forums to build mutual awareness of achievements and open a dialogue
Given the lack of opportunities to-date for ERNs and Companies to enter into dialogue openly, it might make sense to create a dedicated once-a-year event for ERNs and Industry, for the latter to learn more about what ERNs are really doing and see where their strengths lie. This would be a relatively simple but important ‘catch-all’ activity, to help shape more specific collaborations. This is based somewhat on the idea of the Accelerate example, and also on the EURORDIS RoundTable of Companies, but in this option would be envisaged as a single forum for all Networks and all interested Companies to attend. It may be that such a meeting could be part of the EC-organised ERN conference (assuming these recommence, post-covid), or else could be envisaged as a standalone event. Perhaps individual ERN meetings with Industry could branch-off after the plenary.
Establishing disease-specific (or area specific) multistakeholder forums to advance trial-readiness and prioritise collaborative activities
This is a similar activity to the previous, but here fora would be ERN-specific. Multistakeholder groups/fora, organised at more disease-area-specific levels, could be very beneficial to accelerate the pace of trial-readiness and maturation: a good example here is the Accelerate initiative, where all stakeholder, including Industry, gather to discuss the state of the art and identify strategic needs and gaps in their disease area/intervention. Accelerate organise such events for paediatric cancers, but specific fora could be established under the aegis of ERNs, perhaps funded by companies, with the programme created by academics and patients. Forums like these could address some of priorities this WG identified, in terms of ERN: Industry interactions, such as what patient-centred trials in that area look like, agreeing relevant endpoints for studies in X and Y diseases, etc.
Establishing a ‘match-making’ forum for researchers to pitch their ideas to companies and bid for funding support
The case study of the French POC (Proof of Concept) is a good model for this sort of activity. There are certain requirements, if the POC would be replicated in other countries, or indeed established as a vast all-ERN opportunity. This would differ from the activities above, as here, specific research proposals from academics would be presented and assessed. If expanded to the ERNs, it is difficult to see how this would work on a national level; in France, the presence of French Tech Transfer Offices has been crucial. Perhaps a pan-European entity such as EATRIS or other similar body could play such a role, if POC events were organised along ERN lines. The role of the Foundation Maladies Rare here has been critical in the French POC example, as a ‘Neutral and trusted third party’ to initiate and facilitate the partnerships (over the first 5 years, 85 projects have been presented to Industry through the POC Club, with 70 connections made, and an 80% interest rate from the Industry participants)
Enabling assessments of clinical trial feasibility and/or finding patients for clinical trials
A number of activities can be identified which collectively help to de-risk clinical research in rare diseases for Industry. Registries can play a key role in this as (anonymised, aggregate) data can be provided to Companies to help them assess the feasibility of a study in a given condition, with particular inclusion criteria, in particular countries or regions. e.g. the TREAT-NMD case study shows us how registries have been used to inform Companies about the number of patients in particular countries or regions with a particular type of Duchenne Muscular Dystrophy, for instance, within a certain age range, who meet particular inclusion criteria (e.g. are still ambulant, have not taken steroids etc). The aggregate data provided by the national registries associated to TREAT-NMD can then be used to help that Company plan its trials effectively. See further the ‘Registries’ sub-group table. Another useful asset here is TREAT-NMD’s CTSR (Care and Trial Site Registry), which is a registry not of patients but of sites, providing information on those sites, the cohorts they can provide, etc. Some ERNs have developed (and others may be developing) registries able to support with finding patients for trials – indeed, the ERK-Reg case study can perform such a role.
Naturally, any activity aimed at indicating to Companies how many patients they might be able to recruit for research and where they are based needs to be kept separate from actual recruitment efforts (but again, the case studies gathered by Together4RD ensure this a matter of good practice)
Providing expert, tailored and confidential advice to companies for optimised therapy development
Several case studies demonstrate the importance of this function, which, when provided within disease-specific fora, seems to have a major added-value beyond the sorts of early advice offered via Regulatory bodies alone, for instance. For instance, ITTC (Innovative Therapies for Children with Cancer) assesses the relevance of mechanisms of action for experimental paediatric oncology medicines and – if there is potential in the therapy – provides advice to a company on a 1-2-1 basis, ranging from early portfolio evaluation (preclinical) through to support for trial implementation. Having ITTC established as a non-profit legal entity (under French law) has facilitated this service.
The ACT (Advisory Committee for Therapeutics) model, which originated from the TREAT-NMD case study, was also presented as a good (and very replicable) model here. Work is ongoing under the EJP RD to try to take this model, used for over a decade in the neuromuscular field and apply it (with any necessary adaptations) to other RD areas, strategically overseen by ERNs wherever possible. Several fields have expressed interest. However, some form of seed funding is really required to do this well, until the model is established and becomes self-sustaining. Companies could foreseeably look at precompetitive funding of some kind (or if they know they will wish to use the services of an ACT in a given area in the near future, they might consider funding the initial costs.) For many years, the Neuromuscular ACT was run from a single University, which oversaw the contracting etc and used fees from Companies (on a sliding scale, depending on size of the Company) to pay for costs of the panel review meetings. In the absence of a new legal entity, this model could be replicated in ERNs by channelling contracting through a single HCP playing a leading role in the ACT for that ERN. In recent years, largely though the EJP-RD, the ACT model has been expanded to other disease areas, including rare ataxias and the brain tumour community. The ECET (European Collaboration for Epilepsy Trials) is also starting to provide a trial advisory service in the epilepsy field. It is of course essential that such expert advice services maintain confidentiality for the Companies seeking them – the resources names above have developed templates and CDAs (indeed full toolkits, in some cases) which could be used here.
Creating/Improving biobanks
Some communities have their own disease-related biobanks. Other samples are part of very large biobanks and networks of biobanks e.g. EuroBioBank. Projects like RD-Connect embraced the EuroBioBank network and created a biobank and registry finder. BBMRI also maintains a biobank catalogue. It may be, however, that many fields are not using biobanks effectively and would benefit from support to do so.
Diagnosing patients for clinical research through EHRs from ERN centres (HCPs and ‘affiliated’ centres)
Together4RD has not yet received case studies of this happening; indeed, it is likely that this falls into the category of ‘new activity which would be possible between ERNs, specifically, and Industry’. The fact that each ERN connects HCPs across the EU and EEA countries should, in theory, make it more feasible for electronic health record (EHRs) to be federated somehow, to enable the diagnosis of patients not currently diagnosed and enrolled in registries etc. There would be potential for AI approaches to be incorporated here. However, the scope of such activity would require careful consideration: if patients are coming to the attention of ERN HCPs, is it likely that they will remain undiagnosed (and if they are, would AI algorithms be able to solve these cases, or would referral to Solve RD or similar not be more promising?). To really optimise a diagnostic yield of previously undiagnosed patients, perhaps one would need to access EHRs in more general hospitals, rather than specialist clinics, or even in primary care settings. (NB: the Screen4Care IMI 2 project is exploring routes to early diagnosis of people with a RD, through Newborn Screening but also other routes – their work should be illuminating here, perhaps). Therefore, perhaps the added-value here would be less about diagnosing patients who do not have a diagnosis and rather finding patients with particular phenotypes, e.g. stratifying cohorts.
Supporting educational events, to impact the sharing of good practices in diagnosis, treatment, care or research
There is a major need for better educational resources and training in the rare disease field. Some activities in the ‘educational domain could be particularly suitable for ERNs and industry to collaborate on. Examples of educational activities in rare conditions, which receive industry support whilst avoiding conflict of interest, are the masterclasses initiated by TREAT-NMD whilst still coordinated by Newcastle University and now handled by the legal entity which spun out, TREAT-NMD Services Ltd. In 2018 a TREAT-NMD Education Committee was established, comprising both academic and patient experts affiliated with TREAT-NMD who share an interest in supporting educational events for the neuromuscular community. This Committee ensures the independence and appropriateness of all activities endorsed by or delivered by TREAT-NMD, as well as the quality. Companies are able to financially support masterclasses in conditions including Duchenne Muscular Dystrophy, Spinal Muscular Atrophy and Limb-Girdle Muscular Dystrophy. These could be dedicated to professionals in particular countries or regions, to help build capacity around how best to diagnose patients and manage their care. Or they may involve experts from many countries and focus on particular elements of high-quality care provision, such as physiotherapy practices and how to measure and monitor outcomes. Companies value the ability to spread good practices and build professional capacity in conditions they are interested in, and they also benefit indirectly in the sense that such activities will raise -and help to equalise- the standard of care across countries and regions, which is advantageous when it comes to delivering multinational clinical trials and benchmarking.
The ERNs are very much committed to advancing training and education, in various ways. All networks deliver webinars on particular conditions or topics relevant to their ERN domain, which support the sharing of best practices. In addition, ERNs participate in training exchanges, in which staff from some HCPs are funded to visit more experienced centres within the Network, to deepen their knowledge and learn new skills. This exchange programme has been operated by DG SANTE to-date.
Together4RD is not aware of Industry engagement in any of these ERN-led activities to-date, but there may be potential here for unbiased and independent agenda-setting, supported under the right conditions by a company/companies. Another category of education and knowledge generation, more specifically, concerns the creation of clinical practice guidelines.
Generating clinical practice guidelines or clinical decision support tools
An important duty of all ERNs is to generate, update or endorse clinical practice guidelines (CPGs) or clinical decision support tools. A dedicated Tender from DG SANTE supported the creation of many new sets of CPGs, whilst also facilitating the review and possible updating of existing resources. Whilst it would not be appropriate for a company to directly fund a guideline which would recommend use of its own therapy, there could be a role to support this kind of activity less directly, which would be of interest to companies wishing to both improve the level of care patients receive, and ‘level’ the standard of care across countries (both of which can be very important for multinational clinical trials which could otherwise involve patients with very different phenotypes at baseline, purely based on varying approaches to diagnosis, treatment and care from one country to the next.) This might take the form of funding key meetings, e.g. in-person consensus-building meetings to agree on the content of the eventual guidance, or of supporting translations of guidance, once finalised, in different language. Another beneficial activity could be for companies to fund the generation of a lay-person version of the finalised and published scientific guidance (thus removing any suggestions of commercial influence on the contents and recommendations relating to specific medicines). The Together4RD consultation process identified limited examples of such activities but it may be something for ERNs to discuss – perhaps this kind of activity would be especially appropriate for ERNs and Learned/Professional societies to work on together.
One obvious activity in which the two parties may engage are clinical trials, especially as there is a particular need to stimulate more clinical trials in Europe. The Draghi report on ‘The Future of European Competitiveness’ highlighted declining EU competitiveness across several key areas1 calling for stakeholders to “boost the attractiveness of the EU for conducting clinical trials and to expedite access to markets for novel medicines.” (p.31). And a recent EUCOPE (EU Committee of Pharmaceutical Entrepreneurs) report highlights the fact that although Europe remains popular for early-stage investment, later stage clinical investments are continuing to decline, as the EU continues to lose ground to the US and China. It is therefore essential that clinical trials continue to take place in Europe, especially in rare conditions where the unmet needs are so significant (and increasingly, it seems that the traditional, RCT model of clinical trials, will need to be supplemented or substituted for more innovative and adaptive designs and a broader concept of ‘evidence’ (whilst retaining the necessary safety and quality standards for bringing a therapy to market)). The role of ERNs, specifically, in partnering with Industry for better and more numerous clinical trials in rare disease and highly specialised healthcare, has yet to be fully determined; one reason being, the HCPs which are directly part of a given ERN, either as full members or as ‘affiliated’ partners of various formal categories, will always, of necessity, be limited. The vision of ERNs -at least for the larger countries- was not to directly engage every centre or unit with expertise in rare disease across the EU, but rather to engage key players who could then engage other expert units or centres within their country – a so-called ‘hub and spoke’ model. Clinical research focusing on rare conditions typically needs to recruit as many patients as possible, to reach viable numbers for whatever type of trial is intended: and this will surely include reaching out to centres ‘outside’ of an ERN, rather than solely targeting patients visiting the centres which are directly part of a given Network. Therefore, it may not always be possible or even desirable to envisage clinical trials being delivered solely across ERN HCP sites.
The principal goal of Together4RD is to stimulate scientific collaborations between European Reference Networks (ERNs) and Industry. Achieving this goal entails overcoming a variety of historical barriers hampering interaction in this space, by adopting a multi-pronged approach which includes practical support for collaborations, as well as policy and advocacy. A key pillar of the activities in Together4RD centres on launching pilots. In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualising and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized below, and key lessons have been distilled from each pilot, covering positives and areas of innovation for these pilots, whilst also highlighting ways in which these kinds of collaborations might be improved in future ERN-Industry activities.
NB: it is important to remember that these are true pilots, in every sense: this is really the first time ERNs have openly collaborated with Industry, in transparent public collaborations. In multiple respects, these pilots represent very new ways of working, for both Companies and the non-Industry partners; therefore alongside the plaudits that should undoubtably come from actually having managed to launch three tangible projects, there is – as anticipated- a plethora of valuable lessons, which should be shared widely (as many of these not only elucidate some of the challenges in attempting to form public-private collaborations, broadly , but also introduce issues specific to ERNs).
A set of more concise recommendations, distilled from these extensive learnings, are included in this Toolkit as Tool 10 ‘Key Recommendations for both ERNs and Industry from the experiences of the first ERN-Industry pilots’
For a summary of what each pilot is addressing, see here.
Related Resources
Based on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resourceThe first Together4RD pilots resulted from an open call launched in summer 2022, inviting all ERNs to submit an expression of interest outlining proposed industry collaboration, added value, readiness, involved centres, and any existing assets, data or infrastructure to build upon.
View this resource Bookmark this resourceA call was launched by Together4RD in mid 2022, explicitly seeking pilot research project ideas on which at least one ERN and one company could collaborate. These proposals could be submitted, in the first instance, by either ERNs or the companies sponsoring the Together4RD secretariat. Several proposals were received, and after discussions to assess their feasibility by the T4RD Steering Group and facilitated by the secretariat, and to shape ideas into clearer proposals, three pilots were selected for deployment. As it turned out, the initial applications for each of these eventual pilots were in fact submitted by Industry partners. Before drilling down to what worked well in the project initiation phase, for each of these pilots, and where there is room for improvement, it is helpful to explore the different routes each of the pilots have taken, towards their respective launch.
TTP Pilot: Takeda & ERN EuroBloodNet
Takeda submitted a short proposal outline to the Together4RD secretariat, which then formally connected them with ERN EuroBloodNet, the ERN in which expertise in the condition Takeda were interested in here -TTP (Thrombotic Thrombocytopenic Purpura) – would most naturally suit Takeda had performed such a mapping exercise to better understand the patient journey and elicit where the gaps are for patients in the healthcare ecosystem back in 2022 and drafted several possible projects to address the unmet needs identified, which they brought to a hackathon of external stakeholders. This all proved a useful background for approaching Together4RD and the EuroBloodNet team.
From the ERN, the key actors in the pilot are experts in the University of Milan, and the EuroBloodNet research coordination team. They had forged strong connections with the coordination team of the ERN, particularly around a shared interest in using AI to improve diagnosis, and had had some interaction with Takeda in previous years (although not the individuals they ended up working with). Therefore, when the Takeda team submitted the initial proposal to the Together4RD secretariat, the latter was able to facilitate interactions with the ERN.
RHINE Pilot – Novo Nordisk, ERK-Net and Oxal Europe
Similarly, in the case of the RHINE pilot, in rare renal disease, the initial impetus came from Novo Nordisk, who submitted a proposal on Primary Hyperoxaluria (PH). They saw great value and potential in the ERKNet registry, known as ERK-REG, despite it being relatively new (for instance, they were aware that there had already been publications from the registry, and it had been widely presented, which assured them of the research potential). Although an older registry also collected data on PH patients, run by Oxal Europe, there was no real collaboration between those resources, preventing the field from consolidating precious data. Novo Nordisk was initially interested in understanding the barriers to diagnosis for the PH patients, and how this can happen earlier, and then explore what ‘best care’ looks like for people after they receive that diagnosis. A collaborative project with the ERN and the pre-existing registry thus seemed a good opportunity to understand clinical care pathways and the patient journey in rare renal disease but also to harmonise registry efforts for an ultra-rare disease. The Novo Nordisk proposal came about through discussions across the public affairs and medical affairs teams, and once Together4RD brought in the ERN coordination team, that proposal was further co-created with ERKNet and Oxal-Europe to forge a concrete, innovative and mutually beneficial project.
Rare Bone Pilot – Sanofi and ERN-BOND
Here again, the initial proposal came from the industry partner, in this case Sanofi. Sanofi has extensive experience in building registries and in this proposal, they were interested
to explore the extent to which the registry held by ERN-BOND contained adequate and appropriate data to enable a better understanding of the rare bone disease landscape. A particular goal was to better understand the natural history and burden of Osteogenesis Imperfecta (OI). The opportunity of a pilot project was identified by the public affairs and research advocacy teams and brought to the medical affairs team (which explores the wider ecosystem within rare disease, and identifies opportunities to collaborate, whether with patient advocacy groups or academic groups). The coordinator for ERN-BOND was a key opinion leader in the OI field, and had been involved in running registries for many years. The Together4RD secretariat helped to make contact with the coordination team, and a number of discussions exposed the opportunities to utilise the registry that would benefit of both ERN-BOND and Sanofi.
In the RHINE pilot project, the actors were efficient in isolating a precise research question centred on PH. The initial proposal by Novo Nordisk did not contain too much detail but entailed bridging previously distinct registries (the ERK-Reg plus the long-standing registry run by Oxal-Europe). The RHINE consortium did consider a different primary research question to the one it ended up with, which was more concerned with what delays the diagnosis in another disease might cause. This was something Novo Nordisk was keen to explore; however, neither of the registries could really elucidate that, with the data they currently had. Therefore, the partners decided to elucidate the patient pathway and the time from someone being registered as a person with a rare renal disease, to the point when they are diagnosed with a specific subtype, and what specialists they would then consult.
A turning point in agreeing a central research question to shape the RHINE project was that the parties all agreed that as this was essentially a proof-of-concept project, the plan had to be achievable within approximatively a year, and thus they should aim for concrete, deployable and meaningful project objectives without being overly ambitious. The consortium decided not to merge the existing registries, but to combine datasets, through a retrospective data approach. This simplified some of the next steps, such as establishing a governance board involving the 3 organisations involved, and facilitated contracting discussions.
The ERK-NET coordination team brought the proposals to the scientific committee and the registry board, to ensure buy-in of the wider ERN.
Nevertheless, the process of finalizing the proposal still required patience all round:
“The final project scope reflects a middle ground after
numerous revisions”.
In the TTP pilot, some of those involved in the pilot initiation felt that although all parties were agreed that there was scope to collaborate around TTP, drilling-down to a primary research question and project plan was challenging, partially because those involved could identify so many challenges to address.
For the rare bone pilot, Sanofi came with several research questions they wished to work on with the ERN, supported by insights from medical colleagues. However, their representatives were very aware that those questions needed to align with what the ERN partners were interested in exploring:
“If our questions were not aligned… or if we were not willing to change them or work together, then I think it would have been a less successful agreement on those research questions and the scoping.”
The very fact that three pilots successfully launched, after years of very notable and much- bemoaned inactivity between ERNs and Industry, is itself a major positive. However, all three pilots highlighted more specific ways in which these pilots have broken new ground and offer major added value.
Several industry representatives emphasised that the call for proposals came at a perfect time for them, offering fresh opportunities “to build a brand-new collaboration” in fields and areas which perhaps were ‘less-well-trodden’.
All three companies were keen to emphasise that they viewed these pilot projects as the start of, hopefully, long and fruitful collaborations with the ERNs concerned:
“[We will] start in a humble way, but with a great ambition”
For instance, some industry experts noted that entering into more co-creative partnerships like this in the future is very much the way forward, and offers advantages over the traditional one-directional (and purely transactional) approach. Those interviewed noted the enormous potential to understand each other’s strengths and find common interests, and enrich research. The overwhelming learnings from one pilot project initiation have been that this is all about breaking new ground and trying new approaches to get ERNs and industry working together. And naturally, this has meant that some things have not gone to plan – or rather, some steps of the project initiation process could have been conducted more efficiently. But this can be viewed alongside positives; for instance, most of the parties interviewed responded that a good level of trust had been built-up over the proposal preparation process.
Other company representatives were also keen to emphasise that “there was no cookbook here”. Ways of working together had to be figured out, step-by-step. Nonetheless, they highlighted, as major positives in the experience, the excellent relationship established, citing transparency and the absence of any hidden agendas. Where there were uncertainties, these were mutual, so that helped to cement a real partnership.
The academic experts these projects seemed to appreciate the fact that the companies could, and should, have a say scientifically, on the course of project proposal. In some cases, especially, they really highlighted the scientific advantages to working with industry. For one thing, there is a recognition that companies like this can bring greater impact to academic research, and faster. Scientific research is obviously important, and is traditionally the ‘bread and butter’ of researchers: but industry have experience of putting in place methods, strategies, and tools, globally, and managing discussions with regulators and HTA bodies to help ensure the impact of the scientific research the ERN experts wish to do. And all of this was -at least by the time of these interviews, when all parties had been working together for some time- understood and appreciated. This was very important, as for partnerships to be fruitful and trust to be built, all actors need to appreciate the broad expertise and experience each other can bring: in the case of public-private interactions, it is especially important that the industry partner is not viewed merely as a ‘bankroller’ for the research, who should not have a say on the scientific direction, as explained further below.
For their part, even before this Together4RD-initiated opportunity, Novo Nordisk colleagues familiar with ERNs saw great value and potential in the ERK-NET registry, in particular, even though it is still relatively new. Takeda highlighted significant advantages in working with EuroBloodNet, as an existing ready-made network, is highly beneficial, as it offers the possibility to more easily pool enough data to train an algorithm for AI.
There was a sense across all pilots that collaborating with ERNs should bring major efficiencies for companies working in highly specialised fields:
“If we want to do things around diagnostics or education, any existing network is really important for us. [Rare disease areas] may be better taken care of by an existing network collaborating with pharma rather than pharma kind of building from scratch every time”.
Besides the convenience of having a read-made network, several participants highlighted other important advantages of working with an established community like an ERN. This is a departure from the norm, in some ways, as here, Industry isn’t assembling its own bespoke group of experts; instead, the experts are already there and are being proposed, in a sense, to the Company. This is obviously desirable, as the expert base is much more likely to be unbiased. The openness of this approach, therefore, is very beneficial, although, because it is a new sort of approach, it is not without its challenges (as below).
As another added value, several industry respondents mentioned that engaging in these pilots has raised awareness about ERNs internally. The companies involved in these pilots
are large, with a global footprint, and although those engaging directly in Together4RD, as sponsors of the initiative, were of course familiar with the networks, they appreciated the fact that many of their colleagues were not at all aware of ERNs, what they have achieved, and what their potential is.
The interviews with pilot participants also highlighted the fact that different actors within the same ERN also value the collaboration structures these pilots have set in place. One expert reported that it was very positive that the coordination team of the ERN was engaged, as they felt able to focus on the scientific components of the project planning, and not worry about legal and bureaucratic issues that wouldn’t sit within their usual area of expertise. It is worth pointing out that, for all ERNs, researchers in the many HCPs which make up each ERN are still very much getting to know one another professionally, and these kinds of activities really help to iron out the way in which ERNs can operate to support this sort of work. For example, it need not be the case that the scientific expertise in the particular project being proposed actually sits in the coordination team of the ERN – they might have expertise in different conditions under that ERN’s broad heading, and thus it is necessary to bring in experts from other ERN centres, to make the consortium robust.
Related Resources
Together4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceThere have been many positive lessons learned in the conceptualisation and initiation processes of all three pilots; however, those involved in these pioneering efforts also highlighted where there might be room for improvement. In seeking to share some of these learnings, it is important to emphasize that these issues are often not black and white, stemming from the actions -or lack thereof- of one ‘side’ or the other. Indeed, interestingly, sometimes both the academic/clinical experts and the Industry experts identified the
same issues as ‘needing improvement’ but saw room for improvement in addressing these challenges, from both sides.
These pilots – and ERN-Industry activities, generally – represent a departure from the norm
Generally speaking, companies are figuring out how to work with ‘the ERN’ as opposed to with a single academic centre, seeking to clarify where the difference lies (especially as each ERN is not a legal entity). Although the industry colleagues more used to working at EU level, with understanding of the rare disease research ecosystem, were keen to collaborate with the ERNs, some admitted that they needed to advocate internally to convince some of their colleagues of the added-value here, educating them on the status quo of the networks, and what the vision for their company could be. In the case of the non-industry parties, they are either learning how to work with industry for the first time, or else are ascertaining how to work with a company as an ERN, above and beyond any experiences they may have had in an individual PI or university hospital capacity.
When facing new ways of working all round, it is not surprising that new uncertainties and barriers to efficiency are encountered. Representatives from the industry partners explain that companies have processes in place to seek out and strengthen collaborations (or ‘partnerships’, as one respondent prefers to call them). As explained by the interviewees, companies typically award a grant to an expert centre/PI, approaching them with a set of research questions for them to address and publish on. Another classic form of public-private engagement centres around clinical trials. But many of those interviewed, from both industry and academic institutions, emphasised that these are all situations where a company is seeking specific expertise from outside their company. Occasionally this drive comes from the other direction, i.e. someone proposes to the company to run a research project that might actively benefit that company. But either way, traditionally, interactions have tended to be a transactional one-way-street, and to have relatively specific goals.
In these pilot projects, however, although the initial proposals came from the Industry partners, the project plan had to be developed and agreed in a co-creation process -which was sometimes lengthy – involving all parties, which was consequently often marked by a key question: ‘who is really leading and pushing things forward?’ Industry was a partner at the table, rather than a lead – intentionally so, to make each pilot genuinely collaborative.
A robust co-creation process is essential
As above, the pilots all demonstrated that a robust co-creation process is crucial to build a concrete project plan and agree a mutually beneficial research question. Those involved in the pilots wanted a co-creation process in which all parties contribute to the development of ideas, to turn initial proposals into feasible and meaningful projects aligned on the strategy, the expectations and capabilities of all parties involved.
“Although we may have ended up with slightly ‘safer’ research questions than we might usually have gone for, it was essential for all parties involved to feel comfortable with these, and therefore it was a good compromise.”
The most effective approach, from the feedback received, was to genuinely shape the documents and plans together with an iterative co-creation process. The industry parties involved in the pilots welcomed ERN experts providing input during the co-creation process; indeed, in some cases, more vocal input would have been welcomed, e.g. to hear the academics more explicitly stating their ideas, their needs, what they would like to do.
Finding common ground can be challenging. One key insight from the interviews was to focus research questions on unmet needs that go beyond specific therapies—prioritising
a deeper understanding of the disease itself to drive progress. However, public and private partners, while working toward the same goal, may have different priorities for these projects. It’s essential to recognise these differences early on and either accept them or find a way to ensure all parties achieve their desired outcomes.
Avoiding assumptions around public-private collaborations
There are many misconceptions, and unrealistic expectations surround public-private collaborations and interactions. These are not all specific to ERN-industry interactions, but all three pilots shed light on the importance of understanding the perspectives and needs and realities of other stakeholders within a multistakeholder interaction, to make collaborations more fruitful and try to minimise misunderstandings and frustrations. From the interviews, it was clear that the parties involved in the pilots did not feel they were all ‘speaking the same language’. Overall, the pilot initiation process had some major positives, especially in building trust between industry and non-industry stakeholders. However, it took time for everyone to fully understand each other’s priorities and needs.
Early on, there was sometimes a tendency to oversimplify the other side’s motivations. Some of these issues stem from differences in the way in which companies, hospitals and universities are established, and what fundamentally drives them. For the academics involved in these kinds of pilots, there should be a recognition that companies naturally want to diagnose as many patients as possible to maximise the market for their product. However, an industry representative reported feeling that the ERN collaborators initially perceived that company to be driven solely by a desire to sell a product and failed to recognise that some companies “[genuinely prioritize] working in a different way and… really want to address health care ecosystem gaps”.
The takeaway message is not as simple as ‘ERNs need to understand what drives industry’ – although this is absolutely a need, the truth is that different companies may have different priorities, and will value different sorts of outcomes. Naturally, all need to make sure their products have the best chance of making a return on investment. However, in the rare disease space, companies genuinely pride themselves on working towards the greater good, on addressing unmet needs, and they naturally want their would-be collaborators to understand their ethos and trust their goals.
From the industry perspective, there is sometimes a sense that academics can be a little too focused on the scientific outcomes, especially around publications, and do not always see the wider route to impact for the knowledge and tools generated. One industry representative reported that the non-industry parties in their pilot were, to the company’s way of thinking, a little too wedded to academic outputs like scientific publications, whereas they initially envisaged as objective to better understand the patient journey, with the ultimate objective of improving it. The reality is that, for those in academia, scientific publications so often remain the foremost mark of achievement and distinction.
A common frustration—seen beyond ERNs as well—is the belief that ERN researchers primarily wish to collaborate with Industry just to secure funding. This perception can hinder the development of strong, transparent, and trust-based relationships.
“I have things in mind [from a scientific perspective] but can’t do that without that money”.
This is not necessarily a problem, nor is it surprising, given that companies have more financial resources than ERN institutions. Perhaps it is fair to say that issues arise when researchers see industry purely as a funding source. There is a common misconception that companies are both willing and able to simply hand over significant budget to academics to conduct research independently, without collaboration. This misconception is unfortunate, as it creates false impressions of the way in which companies can actually expend funds, but -more importantly, perhaps- can serve to work against the collaborative spirit needed in the rare and highly specialised domain, when seeking to promote more -and more effective- public-private collaboration. Industry has a huge amount of expertise and experience to offer in the design and delivery of projects such as these, and the win:win scenario is one in which public actors seek to leverage that expertise, and recognise the added value of working with a company/companies, beyond the (understandable) desire to plug a financial gap, of sorts. It is important to emphasise that the future success of ERN and Industry interactions will absolutely depend upon this message being disseminated and understood, because the reality, unfortunately, is that ERNs are under resourced to do the myriad of things they are expected to do. Funding for registries, in particular, has been far below what is really needed, to make these resources as powerful as they can be. It is therefore natural that the private sector can easily be viewed as a source of redress for these monetary shortcomings; however, Together4RD wishes to emphasize, and promote, and awareness of the wider value industry can bring to a collaboration.
As mentioned above, a real positive for these pilots is the recognition of the diverse expertise housed by the three Companies involved here – they complement funds with an ability, for instance, to connect the academic partners with their own in-house data scientists and real- world evidence experts. Although ERN registries are a wonderful tool, and their respective communities may have rich experience pre-dating the newer ERN infrastructures, some of the companies in these pilots also have experience in building registries, with many lessons they can share.
But in some cases, it took some time for these kinds of messages to really take hold. For instance, the RHINE project found it was important to have Novo Nordisk included as an equal partner on a steering committee, so that their expertise could really contribute to the development of the project.
The importance of keeping on track and ensuring continued progress
One major area where all parties tended to desire improvement concerned the timelines for the initial scoping, proposal discussion, and project initiation phases. Although it is possible to view the lengthy deliberations as positive in some ways, e.g. enabling time for the proposal to improve and become more meaningful (as one respondent explained), the sentiment all round is that this process took longer than necessary. Helpfully, some ways to improve, in future, were identified, but it is important to explore the varying perspectives as to why things took longer than expected, in other to learn from these experiences.
In all pilots, there was a sense that all participants felt that the timelines for moving from the initial project discussion, to agreeing a revised project and research question, to then generating a more detailed project plan, were longer than would be desirable. Industry parties and academics alike reported that industry tended to push the ERN partners forwards. The RHINE ERN partners reported that Novo Nordisk encouraged them ‘with just the right amount of urgency’ and pushing. However: “the expectations around timelines were not the same”.
The industry participants generally seemed to assign these delays to the significant workloads of the academic partners. Some emphasized that delays are not unexpected when working with academics, and the timelines here were not really very different to those found outside of an ERN; however, there was a general consensus that things should move faster in future.
It may be the case that the conditions in which the Companies proposed these pilots originally were not necessarily amongst the top research priorities of the respective ERNs. Although ERNs were established at a high level, to collectively include all rare diseases, this does not automatically translate to all conditions under those broad headings having the same levels of expertise and prioritization amongst the individual experts of the ERN. It may be that the ‘readiness’ for public-private collaborations, or indeed any research project, is not as high for some conditions as for others. The lack of availability of researchers, to engage with the discussions and project planning, meant that one proposed arm for a pilot, around education, was dropped as it was proving too challenging to secure the necessary time commitments. Again, this illustrates the need to be aware that initial research questions and project parameters may change, from first contact to firming up a project plan.
The ERN/academic experts interviewed about the pilots also acknowledged that the timelines from first contact to really agreeing the project focus and then developing a more detailed project plan, have been too lengthy. Some fully appreciate that this was partially due to their own challenges in prioritising the pilot initiation. However, interestingly, some respondents felt that this is more complex simply than ‘industry pushing for a quick agreement and the non-industry parties hold things up’ – and that some delays have resulted from the nature of the processes within companies, and the perception that the discussions can be sometimes repetitive at the expense of action and decision-making. More than one reported a sense that despite the proposals being submitted by the companies, there was some hesitancy to fully commit to developing a plan – several recall sensing ‘a lot of internal deliberation’ from their respective companies. Another cited the fact that, although the ERN researchers could quite readily be identified, early-on in the process, industry contacts tend to be quite changeable. Colleagues one begins discussions with, at the start of a process like this, may not be the same people one is dealing with further down the line, as there is a high staff turnaround in industry. This can make it challenging to build relationships and keep momentum going, as different people need to pick up the discussions second-hand – this is obviously more of a risk, the longer the process takes.
One consequence of protracted project planning and initiation, which future collaborations might wish to bear in mind, is that as one industry expert pointed out, a company’s priorities can sometimes change over time, and individuals working in these companies have very little power over such things:
“Something that may be a priority today, and could be signed off in a timely way, may not still be a priority five years later”
One challenging component of the pilot initiation phase identified by multiple pilot participants, is budget discussions. Some of the ERN partners reported that they were expecting to be told, quite early on, what the company would be willing and able to contribute financially, to support the work, in order to define what they could include in the scientific proposal. They found it unusual that the companies asked them to define the budget, in the first instance, because again, people were used to being told such things for more traditional types of engagement e.g. in a clinical trial, the company contract with the hospital and they already have the protocol and are explicit about what budget is available. Companies cannot dedicate a set amount of funding (in the way a Horizon Europe grant stipulates a maximum budget, for instance), for a scientific proposal to then explain how it will use that budget ceiling. Rather, the detailed proposal should dictate how much funding a Company is able to dedicate, and hence delays in receiving a specific scientific proposal meant budget envelopes could not easily be agreed. However, with the parties sometimes feeling that they did not know what level of budget was actually available (the ERN parties) or what budget would be requested for a revised scope of work (on the company side), it is easy for a ‘chicken and egg’ situation to develop. Therefore, the earlier in the proposal that budgets can be negotiated, the better. But again, there is a lesson here in understanding and appreciating each other’s modus operandi, and it was suggested that budget envelopes should never be the starting point for project discussions, as it is then easy for the project to come across as having a traditional ‘Industry as hands-off funder’ nature.
“It is important to discuss expectations around resource – because expertise, time, people, understanding and budget are all wrapped into the resources, we’re all committing to this”.
Deep-seated issues such as academic workloads, the need for clarity and agreement around budgets, and the relatively high turnaround of staff in the private sector will not be easily changed; however, the impact of some of the challenges behind the lengthy process of agreeing a robust research question and generating a specific project plan may be ameliorated, somewhat, through greater clarity on who is -and who should- be driving these collaborations forwards.
Who takes the lead? The importance of champions or project managers – people to move forwards
Although it is worth emphasizing again that the nature of the call for these pilot proposals could itself be responsible for some of the issues around delays, as explained above, the fact that these kinds of interactions are new for ERNs and industry makes it especially important to consider who is going to drive the process forward and how. In those earlier, traditional and more one-directional interactions typically seen in previous examples of public-private collaboration, the questions of who does what, by what deadline, for what amount of money, were more straightforward. There was a feeling, from both sides, that academic experts and KOLs are more used to working with pharma “when pharma is running the project”:
“When we do a clinical trial, we have timelines and we are kind of pushing, pushing, pushing because, you know, we’re investing 100 million and it’s important it happens on time. And the problem here I think could be that we’re not certain who is really the driver here. And that’s a challenge.”
Several respondents reported a lack of clarity, on both sides around who was really supposed to be driving some of this work, and, consequently, who was responsible for pushing each stage and seeking consensus and action. It is a new experience for some of these non- industry experts to be asked to do the feasibility work, and the calculations. But because these pilots are viewed as a partnership, there is not that strong sense of ‘ownership’ one way or another. This means that it needs to be handled carefully and early, and these discussions aired, ideally through a third party, to make sure that the process is not stalling simply because of uncertainty either around who is supposed to be doing what, or because one partner does not actually have the knowledge, the experience nor the capacity to perform certain activities they have never done before.
All pilots, one way or another, stressed the value of dedicated project management here. In the PH pilot, this was provided by the ERN Coordination Office and was deemed extremely valuable at enabling good progress at a reasonable pace. But all highlighted how important this is, to have someone either within the consortium or within the Together4RD secretariat -which was identified as a major support – or even completely outside. Some of the industry partners felt it would not be wise for the key project management role to sit within the company itself, as it might change the dynamic. Having a dedicated person—such as a champion or project manager—along with a project tracker was seen as essential for future collaborations. This helps all parties identify delays, understand what the consortium is waiting for, and who is responsible, so support can be provided to keep things on track. Without clarity on the cause of a delay—whether it be workload, waiting for input, or uncertainty about a task—it is difficult for others to step in and help.
One learning lesson that is unique to this new situation of ERNs and Industry seeking to work together, as opposed to any and all public-private projects, is that ERNs may need to consider who should be the driver within the ERN: what should that internal ERN process look like? Ideally, in future, it would be good to see multiple centres within a single ERN collaborating on a project with one company, or even multiple companies. Here, ‘the ERN’ part of the partnership will involve multiple experts, playing different roles, in different institutions. This exposes a major change in public-private collaborations involving networks (as opposed to a unilateral discussion Industry might have with a single Principal Investigator in a single University or Hospital). To make this activity an ERN activity, multiple actors need to be involved, and the ERN itself needs to provide support and endorsement; however, the decision-making processes, and modus operandi for this, is not really clear yet, in most -or even all- ERNs. It will be important for consortia to agree, in future, if decisions always need to come from – or be endorsed by- the ERN coordination team, as this could potentially slow things down and make processes less efficient. Perhaps coordination teams should defer some decision-making to other scientific experts involved in the pilot (who very likely may not sit in the coordinating structure). This is arguably an issue all ERNs are grappling with, for many activities i.e. how to avoid all activities needing sign-off and active participation from the coordinator/coordination team, whilst still maintaining something as an ‘ERN activity’ in spirit. In public-private collaborations, as in all ERN activities, it will be essential to get this balance right, and for coordinators to feel increasingly able to delegate key decisions to other members of their Networks, avoiding the whole process of project planning grinding to a halt until they are able to rededicate some time and attention amongst their overwhelming number of commitments.
The value of face-to-face discussions
All parties agreed the benefits of an in-person meeting (1.5 or 2 days) where everyone gathers around the same table and thrashes out what the project should look like. Such meetings were cited as key tools to speed up progress, allow all parties to air their views, understand the views and needs of others, and generally build partnerships as well as more concrete proposals. All seemed to agree that short virtual meetings, every 6 weeks or so, were not sufficient to drive forwards the discussions and really agree a firm research question. In some cases, a face-to-face meeting (or meetings) with all stakeholders complimented separate discussions with specific stakeholders, to build trust and address concerns on a one-to-one basis when necessary (another valuable lesson is the importance of taking the time and effort to build trust with parties who have not worked together previously).
Some chose to begin their F2F meetings by “sharing concerns, ambitions and limitations” and enabling participants to address some of the common misconceptions and prejudices, on all sides, highlighted above:
“Deep diving… only happened when we spent six hours together or eight hours together. It’s very challenging to be able to accomplish that with one hour Zooms with where you really don’t know each other”
Navigating legal issues
As most of the pilots had not yet concluded the contracting phase at the time of the interviews, the learnings here are somewhat limited. The RHINE project was in the midst of this process, however, having advanced relatively easily to contracting due to streamlining the proposal. Data transfer agreements are relatively straightforward here, as only the two academic partners access the data directly. Again, having a dedicated project manager, and being based in an institution which has undertaken contracting with the private sector in the past, has made the process straightforward. The ERN coordination team did mention that it is proving a little more challenging to include their Industry partner in a trilateral contract, which commits all three legal entities involved in RHINE around one study plan (with milestones and budget plan). But they note that this is understandable and not unusual with these sorts of discussions.
Another piece of advice from a different pilot was to avoid allowing legal contacts in the different institutions to discuss these kinds of projects without the key leads being present. The ERN and Industry experts know what they need, and what they’d like to contract, but leaving this to the legal people can bring about a ‘total misunderstanding’ of what is intended, which overcomplicates the whole process and sets everything back.
The recommendations below stem from the lessons learned in the process of initiating the first three Together4RD pilot projects (for the full report, see Tool 9 ‘Experiences and Learnings from the first ERN-Industry pilots supported by Together4RD’. They essentially function as an executive summary of that detailed report.
Approach prospective partners as soon as possible – especially if the project is in response to a call or specific opportunity. This will allow input from all future partners in that very early project idea.
Embrace a co-creative process from the start, when it comes to reviewing and refining proposals and agreeing a research question. If possible, introduce a face-to-face meeting very early in the process, in which all are encouraged to review all the options on the table, in terms of how to orientate an activity, and share their perspectives, needs, and concerns.
Take time to do your research and understand as much as possible about your prospective collaborators:
- for industry parties, if you do not have deep knowledge of the ERN most connected to the condition(s) you are interested in, consider reviewing Tool 3, What are ERNs?.
- For ERNs, take a look at Tool 5: ‘What does Industry need in a collaboration with ERNs?’.
For Industry – consider how best to pitch an ERN-focused project with colleagues internally (who may not have a strong understanding or awareness of ERNs) and ensure a smooth and early transition from policy to medical departments.
ERNs – be realistic and honest from the beginning in terms of how high a priority a particular condition is for your network. Ideally, share and publicise your research priorities as widely as possible. Be open to research out of the usual ‘comfort zone’, to address unmet needs in the field, but try to balance this with your realistic capacity and levels of internal ERN interest and expertise.
Be clear with a shared vision and mission statement at the start to align partners.
Be prepared to compromise and ‘meet in the middle’ when agreeing a concrete research question and firming-up a project plan.
Opening discussion around outcomes and impact early on should help to build transparent working relationships based on trust.
Understand that public and private actors tend to place value on different sorts of outputs.
- Industry – be prepared that ERN parties will likely place significant emphasis on generating peer-reviewed publications. ERN experts, often anchored in academic institutions as well as hospitals, have professional requirements to publish their work, This is an important marker of esteem, and thus publications will likely be a key output for any project.
- ERNs – consider how research can result in wider impact in terms of changing patient pathways and diagnostics practice, and outcomes beyond publications.
- ERNs – it is useful to accept that companies in the rare disease space tend to have goals and vision to improve the wider rare disease ecosystem, beyond simply developing and selling a product.
Do not underestimate the organisational and cultural differences and plan to take the time to understand what each other desires and needs from this collaboration.
Take time to discuss the expertise and skills each partner can bring to the collaboration – this is important, in order to build a fruitful collaboration in which all slides appreciate what the others can bring and to assess the skills across the full consortium (also allowing the identification of any gaps).
Think carefully about a realistic scope of work, depending on the timelines for completion: it may be helpful to view initial interactions between a given ERN and Industry as a proof-of- concept, starting relatively small but still meaningful, as an entry point for more elaborate projects down the line, e.g. once institutions have experience of forging these collaborations.
- Define small quick wins, achievable in a reasonable timeframe.
If it is the first foray into working with Industry for an ERN, accept that there may be setbacks and things may not develop as efficiently as one would wish – focus on the achievement of delving into a new area of activity, and plan for smoother progress on the next collaboration.
ERNs – accept that the Industry partner(s) will wish to have input to the scientific development of the project plan, and should be viewed as an equal partner. Indeed, this should be welcomed, as it will bring significant advantages to the research, as it will give you access to the vast in-house scientific expertise but also expertise in medicines development, HTA, data science, and much more.
ERNs – be prepared to be vocal in co-developing a concrete project plan. Share your expert perspectives at every stage, as the industry partner will be seeking an active partnership with robust input.
Be prepared, in initial discussions especially, to ask challenging questions of the partners in your project – each party should understand the motivations and drivers of the other, and this means all should be willing to state what they would most like to achieve. This is important to build trust.
Do not postpone resource discussions, as uncertainty can cause delays and misalignment in project planning.
ERNs – it is important to have realistic expectation of both the level of resources industry can contribute to projects, and the way in which it does this. Avoid thinking of companies as purely funders of research. Companies are generally unable to dedicate large sums of money, for the subsequent definition of a detailed project plan – in fact it is the reverse: funding can only be found, internally, based on the contents of a proposed plan. Companies do not award funds as unrestricted grants, without any direct involvement.
Developing a concrete project plan as early as possible supports more efficient negotiations around budget and resources widely.
Identify project owners from both industry and ERNs who are sufficiently senior and have budget decision making power.
Agree who will be the key drivers for each stage of the proposal initiation phase and project plan development.
It is highly recommended that dedicated project management time be allocated, to keep all partners on track. Standard progress tracking tools should be used, to agree timelines for each activity, and the project manager should be willing and able to follow-up when deadlines lapse, to keep the project moving forwards. It may be useful to involve external stakeholders (a third party) to support with this.
Regular virtual meeting should be established, to develop the more specific plan and drive the project forwards. However, these should be supplemented by at least one in-person meeting, across a day or two, ideally, to accelerate progress and address any uncertainties and make decisions.
Where projects involve more than one ERN centre, consider how those teams will work together most efficiently, making best use of everyone’s expertise but also helping to keep a project on track. Consider focusing most of the administrative and bureaucratic and legal activity through one centre, for instance, but agree when and how individual experts and HCPs might take the lead to advance elements of the project.
Appreciate that delays can occur, on both side, and that these can cause major inconveniences (indeed jeopardize the project entirely) – both ERN and industry parties should therefore seek to avoid timelines becoming too long, by closely monitoring their progress and considering whether those working on a project are prioritizing it appropriately. In unavoidable periods of delay, it is imperative to maintain robust communication and inform each other of the situation, to manage expectations.
Companies should attempt to maintain key contacts working on any engagements with ERNs – although some staff turnover is normal, it is important for the rest of the consortium to have sight of who they are working with within each company.
Involve legal departments, from both/all sides, as early as possible.
Ensure that when entering into legal discussions, key project personnel are present at initial meetings of respective legal departments, to avoid misunderstandings.
Related Resources
In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceThis tool explains the origins of ERNs and highlights key resources on their conceptualisation, set-up and operations, including the legal documents on which they are based. It also points to reports and recommendations that analyse the achievements and added value of ERNs to date, indicating where there may be room for improvement, and to key resources showcasing the achievements of ERNs overall as well as where to learn more about the achievements of specific ERNs.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceThis resource consists of a list of key questions which should be considered by anyone contemplating a collaborative activity between an ERN (or ERNs) and Industry (whether single company or multiple). The questions stem from the survey initially used to support the selection of the Together4RD pilot projects, updated in light of the the lessons learned from the pilot initiation process.
It is intended as merely a guide, for all parties (public and private), to help stakeholders ensure they enter into co-creation and negotiations with the best chance of success. Specific and realistic expectations are important, to maximise the efficiency of those early discussions, and hopefully avoid some of the pitfalls that can occur and delay or even jeopardize a public-private collaboration. This should be viewed in connection with Tool 9 Lessons Report on the Experiences and Learnings from the first ERN-Industry pilots supported by Together4RD and Tool 10 Key recommendations for both ERNs and industry from the experiences of the first ERN-Industry pilots.
Objectives / expected outcomes of the collaboration
- What are the overall and specific objectives of the project/collaboration?
- How does the proposal link to wider priorities (for the ERN(s), industry, patients, or the broader policy/Research & Development ecosystem)?
- When would you be ready to start?
- What would a reasonable timeline be for this project to be delivered?
- Would it be a one-off distinct project or do you envisage it as the first step in a longer collaboration?
- Would this project be suitable for multiple ERNs and/or multiple companies to embark upon together? Or is it a single ERN-single company collaboration?
- Are any organisations beyond the ERN(s) and the company(ies) going to be directly involved?
- How would you ensure the ERN(s) supports and shapes this, beyond a single researcher or centre (e.g. has this been discussed in the relevant governance boards? Or research working groups or networks?)
- Are there any areas or outcomes of the project which are non-negotiable?
Expertise and Resources
- Is there already any established infrastructure or data on which this project could/ should build?
- If so, who owns this/how can you access or use it?
- If a registry or registries are involved, who owns the data, what kind of data access agreements are already in place, etc.
- What types of expertise and non-financial resources would be needed? (thinking in terms of technical expertise, scientific expertise, training, etc)
- Who, within the planned consortium, can bring each kind of expertise and resource?
- How do you plan to involve patients/ a relevant patient organisation?
Funding
- What level of budget would be required to meet the project goals you have in mind at this stage?
- What would be the key milestones in this project, and what kind of budget would each require?
Process Considerations
- Would one party drive this forward overall, or lead on particular stages/areas of work?
- Who is ultimately responsible for keeping the project planning, and the implementation, on track?
- Do you have commitment from senior leadership in all respective parties, for project sign-off and for financial issues?
- Who would provide dedicated project management time for the project, and how?
- Would the project involve accessing or collecting patient data (and is it retrospective or prospective data)?
- Do you need to engage/access data for a minimum or maximum number of patients?
- Would the project require ethics approval?
- Have you involved legal and compliance teams in all prospective partner institutions? How will you ensure the smoothest possible approvals process?
- What risks would you foresee?
- And what actions could you envisage to mitigate these?
Related Resources
In 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resource- http://www.rd-action.eu/wp-content/uploads/2018/09/Final-Overview-Report-State-of-the-Art-2018-version.pdf 88-91
- https://download2.eurordis.org/rbv/juggling_care_and_daily_life.infographic__final.pdf – the full report is also available
- https://www.eurordis.org/publications/rb-dailylife-results/
- https://www.eurordis.org/publications/rb-dailylife-results/
- See especially part 1 – ‘the EU context’
- https://ec.europa.eu/health/ph_threats/non_com/docs/rare_com_en.pdf
- https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:C:2009:151:0007:0010:EN:PDF
- Regulation (EC) No 141/2000
- https://www.ema.europa.eu/en/documents/leaflet/infographic-orphan-medicines-eu_en.pdf
- https://od-expertgroup.eu/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8717920/
- See for instance https://www.eucope.org/european-parliament-adopts-reports-on-the-revision-of-the-eu-general-pharmaceutical-legislation/
- https://download2.eurordis.org/rare2030/Rare2030_recommendations.pdf
- https://www.rarediseasesinternational.org/wp-content/uploads/2022/01/Final-UN-Text-UN-Resolution-on-Persons-Living-with-a-Rare-Disease-and-their-Families.pdf
- https://www.rarediseasesinternational.org/collaborative-global-network/
- https://www.rarediseasesinternational.org/wha-resolution/
- https://download2.eurordis.org/rare2030/Rare2030_recommendations.pdf – p.112
- https://doi.org/10.1007/s12687-021-00524-5
- See Part 2 of the Together4RD Position Statement https://ojrd.biomedcentral.com/articles/10.1186/s13023-023-02853-9#Sec11
- https://www.efpia.eu/media/676753/cra-efpia-investment-location-final-report.pdf
- https://commission.europa.eu/topics/competitiveness/draghi-report_en#paragraph_47059
- https://www.eucope.org/eucope-and-fti-consulting-unveil-new-report-on-life-sciences-investment-in-the-eu/
- “This is not to suggest that public–private interactions should not be subject to the highest possible ethical and legal standards: the consequences for the whole R&D community, if there is any action that is seen to transgress or act unethically, can be severe and long lasting. What has perhaps been overlooked in past discussions concerning ERNs and Industry, is the extent to which interactions between rare disease clinicians and researchers, on the one hand, and companies on the other, take place every day—and have been taking place, in some cases, for decades, without issue, whilst providing myriad benefits all round.”
- https://www.nejm.org/doi/full/10.1056/NEJMra1612575 and https://www.nature.com/articles/s41436-019-0616-9
- https://ascpt.onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3428
- https://www.ihi.europa.eu/about-ihi/imi-ihi
- Much of this summary comes from the ERDERA website
- https://erdera.org/beneficiaries-and-participants/
- European Commission, Consumers, Health, Agriculture and Food Executive Agency, Rare diseases 2008-2016 : EU-funded actions paving the way to the European reference networks, Publications Office, 2018, https://data.europa.eu/doi/10.2818/578367
- https://ojrd.biomedcentral.com/articles/10.1186/s13023-016-0398-y
- https://www.rd-action.eu/wp-content/uploads/2018/05/Summary-of-RD-ACTION-Support-for-ERNs-2015-18.pdf
- https://health.ec.europa.eu/rare-diseases-and-european-reference-networks/european-reference-networks/establishing-ern_en
- https://pubmed.ncbi.nlm.nih.gov/33733400/
- https://ojrd.biomedcentral.com/articles/10.1186/s13023-023-02853-9 see part 2
- https://endo-ern.eu/wp-content/uploads/2018/12/Conclusions-and-Next-Steps-from-the-workshop-%E2%80%98How-ERNs-can-provide-added-value-in-the-area-of-clinical-research%E2%80%99-1.pdf
- See Rare diseases 2008-2016- EU-funded actions paving the way to the European reference networks (https://op.europa.eu/en/publication-detail/-/publication/fd1f05fc-6def-11e8-9483-01aa75ed71a1)
- https://health.ec.europa.eu/rare-diseases-and-european-reference-networks/european-reference-networks/erns-evaluation_en
- Ibid.
- https://health.ec.europa.eu/publications/rare-disease-european-reference-networks-addendum-eucerd-recommendations-january-2013_en. See also the foundational work upon which the list appearing in the Addenudum to the 2013 Recommendations was based https://link.springer.com/article/10.1186/s13023-016-0398-y
- https://download2.eurordis.org/documents/pdf/Our_vision_on_mature_ERNs.pdf (especially p.30 ‘Disease Coverage of the ERNs’)
- This was a stipulation of the original 2013 EUCERD Recommendations on European Reference Networks for Rare Diseases – https://health.ec.europa.eu/publications/eucerd-recommendations-european-reference-networks-rare-diseases_en. The EURORDIS Recommendations https://download2.eurordis.org/documents/pdf/Our_vision_on_mature_ERNs.pdf (especially p.30 ‘Disease Coverage of the ERNs’) highlight the need for a stronger focus on the conditons which are currently somewhat out of scope, or not receiving the requisite coverage.
- https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2022.832063/full; Hedley, V., Kole, A., Rodwell, C., and Simon, F. (2019) Rare 2030 Knowledge Base Summary on Data Collection and Utilisation for Rare Diseases https://www.rare2030.eu/our-work/ (p. 4-5)
- https://eu-rd-platform.jrc.ec.europa.eu/erdri-description_en
- https://www.orpha.net/pdfs/orphacom/cahiers/docs/GB/Rare_Disease_Registries.pdf
- https://www.ejprarediseases.org/
- https://erica-rd.eu/
- https://erdera.org/
- https://pubmed.ncbi.nlm.nih.gov/35594066/
- https://www.eurordis.org/our-priorities/european-reference-networks/epag/
- https://www.oaepublish.com/articles/rdodj.2021.001
This Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceThe Playbook provides a practical, user-friendly guide to navigating the complexities of data sharing in IMI/IHI collaborative health research projects, outlining key concepts, roles, decision points, common challenges, and strategies to address legal, technical, and organisational obstacles. It encourages early planning, stakeholder engagement, and adoption of standardised best practices to accelerate data sharing and improve research efficiency across multi-partner consortia
View this resource Bookmark this resourceThis resource explains the importance of public-private partnerships or collaborations for the rare disease community, in the light of the needs of the rare disease field and the current climate around research and innovation
View this resource Bookmark this resourceThis resource presents examples of programmes and structures which facilitate public private partnerships in rare disease or a complimentary area.
View this resource Bookmark this resourceThis tool explains the origins of ERNs and highlights key resources on their conceptualisation, set-up and operations, including the legal documents on which they are based. It also points to reports and recommendations that analyse the achievements and added value of ERNs to date, indicating where there may be room for improvement, and to key resources showcasing the achievements of ERNs overall as well as where to learn more about the achievements of specific ERNs.
View this resource Bookmark this resourceThis Tool illustrates how and why ERNs hold so much potential for research. It is based upon content prepared for the Together4RD Position Statement of 2023, and has been updated to include the latest statistics and development connected with ERNs’ research potential
View this resource Bookmark this resourceThis Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceThe first Together4RD pilots resulted from an open call launched in summer 2022, inviting all ERNs to submit an expression of interest outlining proposed industry collaboration, added value, readiness, involved centres, and any existing assets, data or infrastructure to build upon.
View this resource Bookmark this resourceThe consultations and outreach activities undertaken by Together4RD over the course of 2024 highlighted certain issues or topics which, whilst ultimately not exactly fitting the brief for this Toolkit (in the sense of there beingexisting tools, or tools Together4RD could prepare alone, for a 2024/5 launch) they nonetheless deserve a mention here as they are very much connected to the overall mission of Together4RD.
View this resource Bookmark this resourceIn addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceStakeholders sometimes struggle to consider the range of activities on which ERNs and Industry could collaborate, besides the more traditional engagement around clinical trials, or more recently, partnering with multiple companies through the European Federation of Pharmaceutical Industries and Associations (EFPIA), in a large project via the Innovative Medicines Initiative, for instance. This resource builds upon material prepared for the comprehensive Together4RD Position Statement, to present a table listing a broad range of potential projects and activities which might be well-suited to ERN and Industry collaboration.
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resourceThe consultations and outreach activities undertaken by Together4RD over the course of 2024 highlighted certain issues or topics which, whilst ultimately not exactly fitting the brief for this Toolkit (in the sense of there beingexisting tools, or tools Together4RD could prepare alone, for a 2024/5 launch) they nonetheless deserve a mention here as they are very much connected to the overall mission of Together4RD.
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceThis resource presents examples of programmes and structures which facilitate public private partnerships in rare disease or a complimentary area.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceIn addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceconect4children Stichting (c4c-S) is a non-profit, pan-European organisation that supports paediatric clinical research by providing expert advice and trial support services, including feasibility assessments and site identification, for ERNs and other stakeholders. Building on a successful public–private partnership, it mobilises a large network of experts and research-ready sites to improve the efficiency and quality of paediatric trials across Europe.
View this resource Bookmark this resourceThe resource explains that European Reference Networks (ERNs) are a major EU healthcare and research infrastructure that bring together clinical expertise, data and specialised resources across Europe to tackle rare and complex diseases and are valuable partners for collaborative research activities. It emphasises the untapped potential of ERNs to engage with the pharmaceutical and biotech sectors, advocating for greater awareness and public–private partnerships to accelerate rare disease research and development and benefit patients
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceThe resource explains that European Reference Networks (ERNs) are a major EU healthcare and research infrastructure that bring together clinical expertise, data and specialised resources across Europe to tackle rare and complex diseases and are valuable partners for collaborative research activities. It emphasises the untapped potential of ERNs to engage with the pharmaceutical and biotech sectors, advocating for greater awareness and public–private partnerships to accelerate rare disease research and development and benefit patients
View this resource Bookmark this resourceThis webinar highlighted how industry contributes to PPPs beyond funding, and provided attendees with examples of how industry has brought value to research projects conducted with European Research Networks (ERNs) in recent years.
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resourceThis Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceIn addition to these initial 3 pilots, Together4RD has identified multiple case studies in the rare disease arena which may also serve as food for thought for other stakeholders wishing to follow suite and engage in projects
View this resource Bookmark this resourceThis Position Statement analyses the barriers in ERN-INdustry interactions, and explains how Together4RD is seeking to move the needle, by learning from case studies, exploring frameworks for collaboration, and launching pilots to explore how best to plan and deliver multistakeholder interactions addressing real research needs.
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resourceThe first Together4RD pilots resulted from an open call launched in summer 2022, inviting all ERNs to submit an expression of interest outlining proposed industry collaboration, added value, readiness, involved centres, and any existing assets, data or infrastructure to build upon.
View this resource Bookmark this resourceTogether4RD’s Position Statement highlights that although European Reference Networks (ERNs) have significant potential to accelerate rare disease research and innovation, collaboration with industry has been limited due to structural, regulatory and governance barriers that hinder robust partnerships. It calls for strategic action, frameworks and pilot models to enable transparent, well-supported ERN–industry collaborations that harness collective expertise and resources to better address unmet needs in rare disease research and improve Europe’s competitiveness in the field.
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceThis tool explains the origins of ERNs and highlights key resources on their conceptualisation, set-up and operations, including the legal documents on which they are based. It also points to reports and recommendations that analyse the achievements and added value of ERNs to date, indicating where there may be room for improvement, and to key resources showcasing the achievements of ERNs overall as well as where to learn more about the achievements of specific ERNs.
View this resource Bookmark this resourceThis is a summary of important considerations for stakeholders less used to working with Industry, coupled with a selection of resources (webinars, reports, publications) to help convey some fundamental principles and realities for the private sector in contemplating collaborations with ERNs
View this resource Bookmark this resourceIn 2024, the Together4RD Secretariat interviewed key individuals from both Industry and ERNs, about their experiences in launching the first 3 ERN-Industry pilot projects. These interviews were intended to better understand the respective experiences of conceptualizing and initiating these pilots – from who came up with the original idea, to how the project proposals have taken shape, covering activities up to the launch phase (approximately). The main insights are summarized in this Report
View this resource Bookmark this resourceBased on the extensive interviews with stakeholders involved pilot project, a list of recommendations has been distilled, to guide future ERN and industry projects and collaborations
View this resource Bookmark this resource